common dermatological conditions Flashcards
define macule vs papule?
What about a bulla or a nodule?
Macule–> FLAT area of altered colour (ex freckles)
Papule–> solid RAISED lesion <0.5cm in diameter
nodule–> solid RAISED lesion >0.5cm in diameter
bulla–>raised, clear fluid filled lesion >0.5 cm in diameter
types of skin infection based on pathogen type (ex virus etc:)
· Bacterial
- Impetigo
- Cellulitis/erysipelas
· Fungal
- Tinea (mold – dermatophyte/ringworm)
- Candida (yeast)
- Pityriasis versicolor (yeast
Viral
- Shingles - Herpes zoster
- Chicken pox - Varicella zoster
- Warts – HPV
· Parasite
- Scabies
Acne Vulgaris
definition
Cx
inflammatory disease of pilosebaceous follicle
Cx:
- hormonal
- increased sebum production
- abnormal follicular keratinisation
- bacterial colonisation
- inflammation
Acne Vulgaris
- Types
- locations
- complications
face, chest & upper back
Complix
- Post-inflam hyperpigmentation
- Scarring
- Deformity
- Psychological and social effects

Acne vulgaris
Mx
referral?
Retinoids r contraindicatd in breastfeeding & pregnacny
advice, topical therapies, oral therapies,
Referral: Refer to dermatology if multiple Tx have failed
Oral retinoids (roaccutane) (for severe acne)

Psoriasis
types , cause, triggers
Chronic inflammatory skin condition due to hyperproliferation of Keratinocytes & inflammatory cell infiltration
cx: gentic,enviromentsl, immunological
STREP in LAB
streptocoocus, trauma,retroviral,endocrine, pred, withdrawl, infliximab, nsaids, lithium, ace inhib, b blockers

Symptoms and signs of Psorasis
- well demarcated erythematous White and grey scaly plaques, itchy, burning, painful
- 50% nail involvment pitting, onchylosis oil drop sign,
- AUSPITZ sign
- if athropathy involved ( check for those)

ComplicX of Psoriasis
- Erythroderma : exfoliative dermatitis involving at least 90% of the skin surface
- Psychological and social effects

Psoarisis Mx
referal?
General Measure:
- Tx is only to relieve symp than cure
- given them Psoriasis info leaflet
- nail care: cutt nails, acetone free nail varnish, avoid manicure
- avoid triggers, dont smoke, check medications.
- Use emollients (epimax) reduce scale
- seek medical advice ofr unexplained swelling/joint pain
Topical treatment: may take several wks to work, if stopped suddenly may increase risk of relapse.
steroids (hydrocortisone, eumovate) vit D analogue, coal tar preparations, topical retinoids, keratolytics and scalp preparations.
REFFERAL: if after 4 weeks no symp improvment, severe Psoriasis & effecting phycologically>>REFER DERMOTOLOGY for 2nd line Tx
- Phototherapy
- Oral therapies (if severe extensive or systemic inlvolve): mycophenate mofetil, methotrexate, calcinuren inhibitors,retinoids,
Allergic rashes & urticaria pathophys
- Urticaria is due to a local increase in permeability of capillaries & small venules
- A large number of inflammatory mediators (including prostaglandins, leukotriene & chemotactic factors) play a role but histamine derived from mast cells are the major mediator
- This can be induced by immunlogical and non-immunological mechanisms

Urticaria
symp
Ix
Pruritic wheals
Can progress to angioedema and anaphylaxis – see respiratory emergencies
Ix
if cause cannot be identified from Hx, symptom diaries can help to determine the frequency duration and severity of urticarial symptoms

allergic rashes and Urticaria
Severe acute uritcaria/angioedema:
Mx
General measures: avoid trigger factors, avoid trigger medications (nsaids), it is self-limiting w/out Tx
Uriticaria: non-sedating anit-histamines ex: cetrizine
Severe acute uritcaria/angioedema: treat as above & add Oral corticosteroids 40mg pred for 7 days
Anaphylaxis: IM adren 1:1000 (repeat every 5 mins)
cholophenamine
hydrocortisone

Molluscum contagiosum
pearly papules with central umbillication
2ndry viral infection in eczema
complication
Candidiasis
symp, Ix, Mx,
if topical treatment not work?

White plaques on mucosal areas – can be scraped off · Erythema with satellite lesions in flexures
Ix: Skin swabs for MC&S (for yeasts)
Mx: as above for topical tx, If topical tx is ineffective, the infection is widespread or the person is significantly immunocompromised —-> Oral fluconazole

what is this showing?
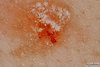
The Auspitz sign in psoriasis
scratch and removal of scales causes capillary bleeding
what is this?
Cx, symp, locations, Ix, Tx

Pityriasis versicolor
Cx: by Malassezia furfur (yeast)
symp: Pale brown/pale patches that fail to tan on sun exposure · Can be scaly/pruritis (Usually asymptomatic)
- can be hyperpigmented, hypopigmented or eryhtmatous
- affects the trunk, neck, and/or arms, and is uncommon on other parts of the body
Ix: Skin swabs for MC&S (for yeasts)
Tx:
General measures
- Advice that it is not contagious as the yeast that causes it is normally present on human skin and infection is not due to poor hygiene
- Treatment is usually highly effective, but may need to repeated as recurrence is common (especially in summer)
- Skin discolouration may persist for several weeks or months following successful eradication
- Vigorous exercise an hour after taking the medication may help sweat it onto the skin surface, where it can effectively eradicate the fungus.
- Bathing should be avoided for a few hours
Medication
- If an extensive area is involved, prescribe an antifungal shampoo
- Ketoconazole 2% shampoo
- Selenium sulphide 2.5% shampoo
- If only small areas are involved, prescribe an antifungal cream
- Imidazole cream – clotrimazole, econzole
Do not prescribe oral corticosteroids

Chicken pox
cause, symptoms, Mx
if immunocompromised?

caused by Varicella Zoster (herpes virus)
- starts of as erythematous papules, ITCHY
- papules become vesicles they may burst
- vesicles crust & scab
- assoc: fever, aches, pains, loss of apetite
General advice:
- most infectious period is 1-2 days before rash appears
- drink loads of fluids
- cutt nails to avoid damage when scratching
symptomatic Tx
- Analgesia
- topical CALAMINE lotion (for itch)
- Chlorphrenamine (for itch in less 1 yr old)
Antivirals:
Oral aciclovir for immunocomporomised adults or teens less than 14 yrs

Scabies
Cx, Epid, symp,tx

Sarcoptes Scabei
Can affect any age group – commonly young/elderly
- Itching is main symptom affecting whole body except head and neck
- Itch worse at night
- Scratch marks and tiny red spots, pustules can develop if crusts become infected
- Mites found in folds of skin webspace and toes, palms of hands, wrists, ankles and soles of feet, groins, and breasts. This leaves tiny spots and coloured lines on skin
Treatment:
General measures
All members of household, sexual partners itching past month and other close personal contacts should be treated, even if asymptomatic
Bedding, clothing and towels should be washed
Medication
Topical insecticide – PERMETHRIN 5% cream
Itching may persist after treatment for up to 2 weeks Medication

what is this?

complication of eczema
painful monophorphic punched out erosions
what is this a manifestation of?

Oil drop sign (onchylosis) in Psoriasis
seperation of nail bed from nail plate
Eczema
describe, epid, causes, location , types, presentation
or dermatitis is a genetic defect in the skin barrier caused by loss of fuction of fliggarin protein.
Epi: mainly is less than 12 yrs old, develops early childhood gets better in teens
Loc: infants >> extensor regions and face/ Adults: flexors and face
Cx: Atopy (asthma, allergic rhinitis), foods, stress, heat, sweating, allergins, pet fur, moulds, dustmite,pollen
Symp: vesicular, itchy, weepy
Types: mild, moderate, severe, infective

what is this?
epidx, Cx, symp, Ix

Impetigo is a skin infection that’s very contagious but not usually serious, common in young kids
Skin swab MC&S, if inconclusive diagnosis or recurrence despite tX

impetigo types
Systemic signs possible in severe cases
Fever, Malaise, Weakness

cellulitis vs erysipelas
Rfx, present, complx,
spreading bacterial infection of the skin caused by Strep pyogenes & Staph aureus
- Cellulitis (l pic) – involves deep subcutaneous tissue
- Erysipelas(R pic) – acute superficial form of cellulitis and involves dermis and upper subcutaneous tissue
Risk factors: • Immunosuppression • Wounds • Leg ulcers • Minor skin injury
symp: May be associated with lymphangitis

Shingles
singles in facial nerve?
Ix

caused by Varicella zoster (Herpes virus), reactivation of chicken pox virus
- Erythematous vesicles and pustules that dry out forming crusts and scabs
- The scabs drop off within 2-3 weeks
- Covers a well-defined area of skin on one side of the body w/out crossing the midline
- Pain may persist long after the rash had cleared – usually goes away in 6 months
Shingles in facial nerve – Ramsey hunt syndrome
Ix: Clinical diagnosis, If in doubt, scrapings from blister for MC&S / viral swab test for PCR
Shingles
Mx
General measures
- Explain that only a person who has not had chickenpox/varicella vaccine can catch chickenpox from them.
- They are infectious until all the vesicles have crusted over
- Avoid contact with people who have not had chickenpox
- Avoid sharing clothes/ towels
- Wear loose fitting clothes to reduce irritation
- Cover lesions that are under clothes while the rash is weeping
- Keep it clean
- Avoid work
Medication:
- Analgesia – paracetamol, codeine
- Oral aciclovir within 72 hours for :
- Age >50 o Immunocompro mised
- Non-truncal involvement
- Moderate or severe pain
- Moderate or severe rash

Rosacea (doha)
epid, cx, symp

- More common in women bur more severe in men
- Affects fair skinned individuals
- Chronic condition that can persist for a long time – severity fluctuates
Cx:
Not fully understood 0 genetics, immune system and environmental factors. Involved
triggers: • Alcohol • Exercise • High and low temperatures • Hot drinks • Spicy foods • Stress • Sun
- Usually affects the face
- Starts with a tendency to blush easily
- After a while, central areas of the face become a permanent deeper shade of red, with small dilated blood vessels, papules and pustules
- Occasionally, there is swelling of the facial skin (lymphoedema) around the eyes
- Occasionally, an overgrowth of the sebaceous glands on nose may cause the nose to become enlarged, bulbous and red – rhinophyma
Describe the rash
if theyre transient (<24 hours)?

GENERALISED SYMMETRICAL rash, consisting of WELL DEFINED, ERYTHEMATOUS, URTICATED PAPULES AND PLAQUES
if we know they are transient (<24 hours) we can call them WHEALS
Describe the 2
causes, epidemiolgy, common areas, secondary symptoms

Pityriasis rosea
is a viral rash which lasts about 6–12 weeks, starts of as a single rash (herald patch) then after 1-20 days may devlop into a generalized secondary rash.
young adults and teens
mainly on chest and back
may be very itchy, but in most cases, it doesn’t itch at all. malaise and headache
- •IMAGE 1: A Single, localized, oval erythematous/pink plaque approx 2–5 cm in diameter, with a scaly collaret trailing on the edge of the lesion àHERALD PATCH*
- •IMAGE 2: Generalized, erythematous, well defined macules/plaques, which are a mix of oval and annular shaped*