Colitis/Colon Tumors Flashcards

Normal colon

Diverticulum; outpouchings of colonic mucosa and submucosa; common in US population (low fiber diet), can be plugged with stool, get secondarily inflammed (diverticulitis)
Active colitis; infiltration of neutrophils into surface/crypt epithelium; usually presents with diarrhea; see cryptitis (neutrophils within epithelium of crypt), expanded LP with inflammation, crypts are further apart than normal though architecture still intact.
“active colitis” is a non-specific finding; can be due to infectious colitis, IBD, or NSAID hyperinflammation

Active colitis; see intraepithelial and intraluminal neutrophils due to crypt rupture

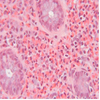
Infectious colitis, see cryptosporidium (blue arrows), pt presents with active colitis, take a travel hx

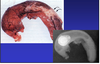
C. diff pseudomembranous colitis; grossly colon appears very erythematous with yellow/green pseudomembranes (made of fibrin, mucin, and inflammatory cells); can lead to sepsis/death

Pseudomembranous colitis; see pseudomemb. replace full thickness of mucosa and are comprised of a “volcano-like” extrusion of mucin, fibrin, and neutrophils.

C diff pseudomembranous colitis vs. ischemia; fibrino-purulent destruction of epithelium with neutrophils; look very similar cannot differentiate under microscope so clinical hx very important

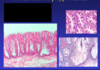
microscopic collagenous colitis; often seen in middle-age women with chronic watery diarrhea, colonscopy is normal, by on bx see lymphocytes, plasma cells, and eosinophils in LP, damage to the surface epithelium with thickening of BM;
on trichrome stain see blue bands of collagen under surface eptihelium.

Microscopic lymphocytic colitis; chronic watery diarrhea seen more often in men, similar to collagenous colitis, prominent lymphocytic infiltrate or crypts, damage to surface epithelium, no collagen deposition; often seen related to drug rxns
Eosinophilic colitis; rare, seen in neonates and young adults, 75% with hx of allergy/atopy, often seen in pt with eosinophilic gastritis/esophagitis; ddx includes parasitic infection, drug rxn, IBD

Ischemic colitis; most cases related to atherosclerosis, pt present with rectal bleeding, abd pain or full-blown peritonitis; on microscopy see slight atrophy of mucosal crypts or even full-thickness bowel necrosis; surg intervention usually necessary
Big photo, on L see remnant crypts, on R see no surface epithelium

Chronic colitis; see crypt distortion/drop-out, plasma cell/lymphocyte infiltrates that broaden separation between MM and crypts, paneth cell and pyloric metaplasia

Crohn’s Dz; may affect all parts of the GI tract, most frequently the terminal ileum, often spares rectum–“Skip lesions”; see transmural (full-thickness) inflammation and fibrosis; can lead to deep fissures, fistulas, and non-casseating granulomas
complications include strictures, fistulas, and local recurrence

Crohn’s Dz; can affect all parts of the GI tract, most commonly terminal ileum, sparing rectum; see mucosal changes of chronic colitis, transmural inflammation and fibrosis, deeps fissures/fistulas, and non-casseating granulomas

Crohn’s Dz, mesenteric fat overgrowth

Crohn’s Dz; see mucosal changes of chronic colitis, transmural inflammation and fibrosis; smaller photos on bottom show non-casseating granuloma

Ulcerative Colitis; rectum always involved, see continuous inflammation confined to mucosa and submucosa, muscular wall nml, no deep fissures/fistulas, “pseudopolyps” common, rare granulomas; complications include toxic megacolon and colitis cystica profunda

Ulcerative colitis, see pseudopolyp with fibrinopurulent debris
Ulcerative colitis; low grade on L, high grade on R

MALT lymphoma—mucosal associated lymphoid tissue, B cell origins, associated with H.pylori infection

MALT lyphoma
Acute appendicitis; lifetime risk 7%, M>F, increased intraluminal pressure and decreased venous outflow, 50-80% due to overt obstruction; leads to ischemic injury, stasis, bacterial proliferation and inflammation.

Acute appendicits, see neutrophil infiltrates

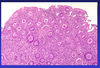
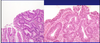
Peutz-Jegher polyps; autosomal dominant dz in which pts have numerous hamartomatous polyps (SB>stomach>colon); arborizing architecture and abundant mucin. Dx’d in childhood, kids with pigmentation on lips, buccal mucosa, hands/feet. Increased risk of CA in pancreas, breast, lung, ovary, and uterus.

Juvenile polyps, most common form of hamartomatous polyp in pediatric patients, frequently presenting with rectal blood/mucus; lesions have large, dilated crypts in an inflamed stroma, often eroded/ulcerated at surface. Usually benign though some forms have hundreds of polyps, related to SMAD4 or BMPR1A genes and have a slightly increased risk of adenoCA.

Juvenile polyposis

Hyperplastic polyps, most common type seen in adults, characterized by elongation of crypts lined by cells producing excessive amounts of mucin. Completely benign
Sessile serrated polyp; dysplastic adenomatous polyp that is a precursor for R-sided colon CA; see dilated crypts

Tubular adenoma; most common variant, retain glandular configuration, can grow in sessile or pedunculated manner. Small risk of adenomCA, should be removed.

Villous adenoma; least common form of adenoma, have long, finger-like extensions that dominate 75% of the architecture; 2-17% frequency of invasive tumor, should be removed.

Early invasive adenoCA; colonic CA most common GI cancer, #2 cause of cancer-death in USA, peak incidence in older ppl, high fat/low fiber diet a RF; presents with bleeding, stool changes, wt loss fatigue.

Colon CA

Colon CA, irregularly shaped glands lined by cells with atypical nuclei and prominent nucleoli, cell necrosis is common

Metastasized colon CA; lymph node #1 site, liver is #2.
Statging (TMN) is most important prognostic factor in colon cancer

FAP, familial adenomatous polyposis; a hereditary AD disorder leading to hundreds of colonic polyps by 25 y.o and 1+ adenoCA by 40’s. Due to mutation in the APC gene, a tumor supressor gene located on chromosome 5

FAP; mt in APC gene that leads to dev. of hundreds of polyps and adenoCA, see dysplastic crypts on LM.

APC mt (FAP) or MSH2 (MMR mutation in HNPCC) is first-hit
KRAS is mt’d in 30-40% of CRC, part of EGFR pathway, makes tumor able to grow and survive, and spread