Chapter 18: Cholestatic Disease Flashcards
Hemolytic disease of the newborn (erythroblastosis fetalis) results in the accumulation of _________ bilirubin in the brain and can lead to _______.
Hemolytic disease of the newborn (erythroblastosis fetalis) results in the accumulation of unconjugated bilirubin in the brain and can lead to kernicterus.
Deficiency of canalicular membrane transporters (i.e., Dubin-Johnson syndrome, or Rotor syndrome) results in which form of hyperbilirubinemia (unconjugated or conjugated)?
Conjugated
Impaired bile flow from a duct obstruction or autoimmune cholangiopathies result in what type of hyperbilirubinemia (uncojugated or conjugated)?
Conjugated
What is the inheritance pattern of Crigler-Najjar syndrome type I?
What is defective and how seriously?
- Autosomal Recessive
- Complete absence of UGT1A1 activity
What is the inheritance pattern of Crigler-Najjar syndrome type 2?
What is defective and how seriously?
- Autosomal Dominant w/ variable penetrance
- Decreased activity of UGT1A1
What is the inheritance pattern of Gilbert Syndrome?
Autosomal Recessive
What is the inheritance pattern of the Conjugated-Hyperbilirubinemias, Dubin-Johnson and Rotor Syndrome?
Autosomal Recessive
Which hereditary hyperbilirubinemia is associated w/ pigmented cytoplasmic globules in the liver?
Dubin-Johnson Syndrome
What are the 2 characteristic lab findings of Cholestasis?
- Increased Alkaline Phosphatase
- Increased GGT (gamma-glutamyl transpeptidase)
What are 2 morphological features common to both obstructive and nonobstructive cholestasis?
I.e., seen in bile canaliculi and hepatocytes
1) Elongated green-brown plugs of bile visible in dilated bile canaliculi
2) Bile pigment in hepatocytes = fine, foamy appearance, with so called “feathery degeneration”

A secondary bacterial infection of the biliary tree that aggravates the inflammatory injury produced by subtotal or intermittent obstruction is known as?
Ascending cholangitis
What is the most severe form of cholangitis and what is seen?
Why is prompt diagnostic evaluation and intervention imperative?
- Suppurative cholangitis = purulent bile fillsanddistends bile ducts
- Sepsis rather than cholestasis tends to dominate, requiring prompt intervention!
What is the histologic hallmark of ascending cholangitis?
Influx of periductular neutrophils directly into the bile duct epithelium and lumen

Surgical intervention is warranted and imperative for which type of biliary obstruction causing cholestasis (extraheptic or intrahepatic or defects in hepatocyte bile secretion)?
- Extrahepatic
- NOT indicated for intrahepatic or hepatocellular secretory failure because the patients condition may actually worsen
What can sometimes become superimposed on the pathogenesis of untreated chronic biliary obstruction and the damage accruing in the liver (i.e., ductular rxns, periportal fibrosis, and hepatic scarrin)?
Can trigger what?
- Ascending cholangitis
- Triggering acute-on-chronic liver failure
Response by the liver to circulating microbial products of which kind of organisms is most likely to lead to cholestasis of sepsis?
What is the most common form?
- Gram-negative organisms
- Canalicular cholestasis = MOST COMMON = bile plugs in centrilobular canaliculi + mild portal inflammation + NO hepatocyte necrosis
Unlike other forms of cirrhosis, nodules of liver cells in biliary cirrhosis often take on what characteristic shape?
Not round, but IRREGULAR, like jigsaw puzzle pieces

Where does Primary Hepatolithiasis (aka recurrent pyogenic cholangitis) have a very high prevalence?
East Asia
What is the typical presentation of someone with Primary Hepatolithiasis?
- Repeated episodes of ascending cholangitis
- Fever and abdominal pain 2’ to infection of ducts
- Sometimes a mass-like lesions may be present and mistaken for malignancy
Primary Hepatolithiasis is caused by a gallstone where and what does this lead to?
Increased risk of which malignancy?
- INTRAhepatic gallstone –> repeat bouts of ascending cholangitis –> progressive inflammatory destruction of hepatic parenchyma
- Increased risk of invasive cholangiocarcinoma
Pigmented calcium bilirubinate stones in distented intrahepatic bile ducts, with chronic inflammation, mural fibrosis, and peribiliary gland hyperplasia, ALL in the absence of extrahepatic duct obstruction is characteristic of which disease?
Primary Hepatolithiasis
Which infants should be evaluated for neonatal cholestasis?
Infants w/ jaundice BEYOND 14-21 days after birth
Why is the differentiation of biliary atresia from nonobstructive neonatal cholestasis very important in regards to treatment?
- Definitive treatment of biliary atresia requires surgical intervention (Kasai procedure)
- Surgery may adversely affect clincal course of child w/ other disorders
Neonatal infeciton by which virus is a common cause of Neonatal Cholestasis?
CMV
What is a characteristic feature of hepatocytes associated with Neonatal Hepatitis?
Panlobular giant-cell transformation of hepatocytes

Biliary atresia is defined as what?
Complete or partial obstruction of the lumen of the extrahepatic biliary tree within the first 3 months of life
What is the single most frequent cause of death from liver disease in early childhood and accounts for 50-60% of children referred for liver transplantation?
Biliary Atresia
What are the 2 major forms of Biliary Atresia and how do they differ?
Which is most common?
- Fetal form: due to ineffective formation of laterality of thoracic and abdominal organs during development —> aberrant intrauterine development of the biliary tree
- Perinatal form: normally developed biliary tree is destroyed AFTER birth (CMV, Reovirus, Rotavirus) = MOST COMMON form
Which 3 viruses have been implicated in the development of the perinatal form of biliary atresia?
1) CMV
2) Reovirus
3) Rotavirus
Morphologically what are the characteristic features seen in the hepatic or common bile ducts of biliary atresia?
Inflammation and/or fibrosing strictures
There are 3 types of biliary atresia based on the anatomy of which duct(s) are involved, which is the most common and is this type correctable w/ surgery?
- Type III - obstruction of bile ducts at or above porta hepatis
- This type is NOT correctable
How does an infant with biliary atresia typically present?
Which lab findings?
- Present w/ neonatal cholestasis (jaundice > 2 weeks post-delivery), but exhibit normal birth wt. and postnatal wt. gain
- Normal stools –> acholic stools (pale/clay colored)
- High serum bilirubin and moderately elevated aminotransferase and alkaline phosphatase
What is the primary treatment for Biliary Atresia?
Liver transplantation or else death occurs within 2 years
Differentiate the age of onset and gender predominance for Primary Biliary Cirrhosis vs. Primary Sclerosing Cholangitis
- Primary Biliary Cirrhosis = between age 30-70 (median age = 50 yo) and primarily women (9:1)
- Primary Sclerosing Cholangitis = age 30 yo and primarily men
What is the characteristic lab finding of Primary Biliary Cirrhosis?
Antimitochondrial antibodies (AMA-positive)
What do the AMA-positive antibodies recognize and bind to?
E2 component of pyruvate dehydrogenase complex (PDC-E2)
Which type of lesion is characteristic of Primary Biliary Cirrhosis?
Describe the lesion.
Florid duct lesion = destruction of interlobular bile ducts by lymphoplasmacytic inflammation w/ or w/o granulomas
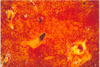
Unlike in drug-induced or sepsis-associated cholestasis where does the bile accumulate in Chronic Primary Biliary Cirrhosis?
Associated with what morphological findings in the liver microscopically (hepatocytes) and grossly (i.e., size and color)?
- Periportal or periseptal bile accumulation (NOT centrilobular)
- Feathery degeneration and ballooned, bile-stain hepatocytes
- Mallory-Denk bodies
- INTENSE green pigmentation of the liver and marked HEPATOMEGALY

How are most cases of Primary Biliary Cirrhosis diagnosed?
Which labs are elevated?
- Diagnosed when patient is asymptomatic
- Present w/ elevated levels of Alkaline Phosphatase and GGT; may also have hypercholesterolemia
How is Primary Biliary Cirrhosis confirmed?
Liver biopsy showing florid duct lesions
If Primary Biliary Cirrhosis presents symptomatically what symptoms are present?
Fatigue and pruritus
With progression of Primary Biliary Cirrhosis, which secondary features/disorders may emerge?
- Skin hyperpigmentation
- Xanthelasmas
- Steatorrhea
- Vit D malabsorption-related osteomalacia and/or osteoporosis
Which 5 extrahepatic manifestations may be present with Primary Biliary Cirrhosis (i.e., other autoimmuen disorders)?
- Dry eye and mouth complex (Sjogren syndrome)
- Systemic sclerosis
- Thyroiditis
- Rheumatoid arthritis
- Celiac disease
Which autoimmune disease is characterized by nonsuppurative, inflammatory destruction of SMALL and MEDIUM size INTRAhepatic ducts?
Primary Biliary Cirrhosis
Which autoimmune disease is characterized by inflammation and obliterative fibrosis of intraheptic and extrahepatic bile ducts with dilation of preserved segments?
Primary Sclerosing Cholangitis
Characteristic “beading” on radiographs of the intrahepatic and extrahepatic biliary tress is associated with what disease?
Primary Sclerosing Cholangitis
Which other diseases are associated and often coexist w/ Primary Sclerosing Cholangitis?
- IBD (70%) –> Ulcerative colitis
- Pancreatitis
- Idiopathic fibrosis diseases
Which HLA molecule and autoantibody are associated with Primary Sclerosing Cholangitis?
- HLA-B8
- Perinuclear antineutrophil cytoplasmic Abs (p-ANCA)
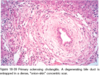
What are characteristic morphological findings in both the involved large ducts and small ducts in Primary Sclerosing Cholangitis?
- Large = similar to UC: acute, neutrophilic infiltration of epi. superimposed on chronic inflammatory background
- Small = striking circumferential “onion skin” fibrosis around atrophic duct lumen –> obliteration by “tombstone” scar
Which symptoms in a patient may signify the development of Primary Sclerosing Cholangitis?
- Progressive fatigue, Pruritus, and Jaundice
- Acute bouts of ascending cholangitis
Patients with Primary Sclerosing Cholangitis who are asymptomatic may come to attention due to what underlying condition and lab value?
Persistent elevation of Alkaline Phosphatase, especially in pts w/ UC and are routinely being screened
Which type of cyst presents as a congenital dilation of the common bile duct and most often in children before the age of 10?
Symptoms?
Which sex affected more often?
- Choledochal Cyst
- Jaundice and/or recurrent abdominal pain
- Females (4:1)
Choledochoceles are a form of Choledochal Cysts that protrude where and increase the risk for what?
- Protrude into the duodenal lumen
- Predispose to stone formation, stenosis and stricture, pancreatitis, and obstructive biliary complications
Which 3 sets of pathologic findings/lesions may be seen, sometimes overlapping with each other in Fibropolycystic Disease?
- Von Meyenburg complexes: small bile duct hamartomas
- Single or Multiple, intrahepatic or extraheptic biliary cysts
- Congenital hepatic fibrosis
Fibropolycystic Disease and its associated lesions are due to what malformations?
This disease often occurs with what other disease?
- Ductal plate malformations –> abnormal biliary tree development
- Often occurs w/ Autosomal Recessive Polycystic Renal Disease
When does Fibropolycystic Disease typically present (onset)?
Most severe forms may present with?
- Late childhood or adolescence
- Hepatosplenomegaly or Portal HTN
Caroli syndrome is used when what 2 findings occur together?
Biliary cysts + Congenital Hepatic Fibrosis
Interruption of the hepatic artery does not usually produce ischemia/necrosis of the liver, BUT what is the one exception?
Hepatic artery thrombosis in a transplanted liver, generally leads to infarction of the major ducts of the biliary tree
What is the most common cause of small portal vein branch obstruction?
Schistosomiasis (trematode/blood fluke); eggs of the parasite cause obstruction
Small portal vein branch diseases are characterized by what?
i.e., what type of portal HTN and injury
- NON-cirrhotic portal HTN w/ portal fibrosis
- Obliteration of small portal vein branches
*Most common cause = Schistosomiasis
What is the most common intrahepatic cause of blood flow obstruction?
Cirrhosis
Which 4 diseases may cause physical sinusoidal occlusion?
1) Sickle Cell disease
2) DIC
3) Eclampsia
4) Diffuse intrasinusoidal metastatic tumor
AIDS-associated peliosis (sinusoidal dilation - due to impedement of hepatic blood efflux) has been associated with what organism?
Bartonella species (gram negatives)
Liver enlargement, pain, and ascites, associated with obstruction of 2+ major hepatic veins is a condition known as?
Budd-Chiari Syndrome
What is the gross morphology of the liver in Budd-Chiari syndrome?
Swollen and red-purple and has a tense capsule

Hepatic vein thrombosis —> Budd Chiari Syndrome may be caused by what underlying disorders and risk factors?
- Polycythemia vera
- Antiphospholipid antibody syndrome
- Paroxysmal nocturnal hemoglobinuria
- Intraabdominal cancer –> hepatocellular carcinoma
*Pregnancy and OC use thru interaction w/ underlying thrombogenic disorder

How is acute hepatic vein thrombosis treated?
Portosystemic venous shunt
Sinusoidal Obstruction Syndrome is most commonly seen in which 2 groups of patients?
1) Post-allogenic HSC transplant (within 3 weeks)
2) Cancer pts receiving chemotherapy
Obliteration of the terminal hepatic venules by subendothelial swelling + collagen deposition + accumulation of hemosiderin-laden macrophages are characteristic of which disorder?
Sinusoidal obstruction syndrome
Left sided heart failure or shock may lead to hepatic hypoperfusion and hypoxia, causing what kind of injury to hepatocytes and in which location?
Ischemic centrilobular coagulative necrosis
What type of injury does the combination of hypoperfusion and retrograde congestion of the liver act synergistically to cause?
Liver takes on what characteristic look?
- Centrilobular hemorrhagic necrosis
- Known as “nutmeg liver”
Vanishing bile duct syndrome is seen in which setting?
What 2 factors cause the injury to the bile ducts?
- Chronic rejection of transplanted liver = Host vs. Graft
- Destruction of bile ducts by: immunologic attack and interruption of blood flow
What is the most common cause of jaundice in pregnancy?
- Viral hepatitis (HAV, HBV, HCV or HBV + HDV)
- HEV runs more severe course and is often fatal
What are the findings in preeclampsia and how what findings are necessary for it to be known as ecclampsia?
- Maternal HTN, proteinuria, peripheral edema, and coagulation abnormalities
- When hyperreflexia and convulsions occur = ecclampsia –> may be life-threatening
Sometimes, subclinical hepatic disease may be the primary manifestation of preeclampsia and is part of a syndrome known as HELLP syndrome - which stand for?
- H - hemolysis
- E - elevated Liver enzymes
- L - low Platelets
In preeclampsia, the periportal sinusoids contain deposits of _______, which are associated with __________ into the space of Disse
In preeclampsia, the periportal sinusoids contain deposits of FIBRIN which are associated with HEMORRHAGE into the space of Disse
What can lead to catastrophic hepatic rupture in patients with ecclampsia?
Dissection of blood under Glisson capsule

Although rare, when does Acute Fatty Liver of Pregnancy present and with what symptoms?
- Third trimester
- Sx’s attributable to hepatic failure –> bleeding, N/V, jaundice and coma
Acute Fatty Liver Disease is unique in its pathogenesis how?
What causes the problems?
- Rare instance of fetus causing metabolic disease in mother
- Mother and Father carry heterozygous deficiency in long-chain 3-hydroxyacyl CoA dehydrogenase
- Fetus or placenta produces long-chain 3-hydroxylacyl metabolites which enter maternal circulation and cause hepatic injury
What is the treatment for Acute Fatty Liver of Pregnancy?
Termination of Pregnancy
Intrahepatic Cholestasis of Pregnancy presents during which trimester?
With what symptoms?
- Third trimester
- Onset of pruritus –> dark urine w/ occasional light stools + jaundice
The level of what is increased greatly in Intrahepatic Cholestasis of Pregnancy?
Bile salts —-> Pruritis
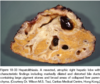
A single well-demarcated, poorly encapsulated lesion w/ central stellate scar; while the rest of the liver appears normal is characteristic of what type of nodule?
Focal nodular hyperplasia
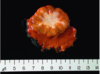
Focal nodular hyperplasia most often arises in which age group?
Young to middle-aged adults
The central stellate scar seen in focal nodular hyperplasia contains what type/size of vessels?
What changes do these vessels show?
Large vessels, usually arterial, that show fibromuscular hyperplasia w/ eccentric or concentric narrowing of the lumen
What is seen in Nodular Regenerative Hyperplasia?
- Liver is entirely transformed into nodules, WITHOUT fibrosis (differentiates it from micronodular cirrhosis)
- Plump hepatocytes surrounded by rims of atrophic hepatocytes
Nodular regenerative hyperplasia can lead to the development of?
Portal HTN
Nodular regenerative hyperplasia occurs in association with conditions affecting intrahepatic blood flow, such as?
- Solid-organ transplants (particularly renal)
- Hematopoietic stem cell transplantation and Vasculitis
- HIV-infected pts
- SLE
What is the most common benign tumor of the liver?
Cavernous hemangioma
How do cavernous hemangiomas appear grossly?
Histologically consists of?
- Discrete red-blue, soft nodules, usually <2 cm; located beneath capsule
- Vascular channels in a bed of fibrous CT
Hepatocellular adenomas are associated with the use of which drugs?
Especially?
- Anabolic steroids
- Oral contraceptives = 30-40x increased risk!!!
HNF1-α inactivated hepatocellular adenomas are often seen in association with what other mutation and how is it inherited?
Most common sex affected?
- Autosomal dominant MODY-3 (maturity onset diabetes of the young, 3)
- Most commonly in women
HNF1-α inactivated hepatocellular adenomas carry what risk of malignancy?
How can they be stained/identified?
- Devoid of atypia –> almost NO risk for malignant transformation
- Immunostaining for LFABP
β-catenin activated hepatocellular adenomas have what risk of malignant transformation?
How should they be handled?
Associated w/ what risk factors and sex?
- Very high risk for malignant transformation
- Should be resected even when asymptomatic
- OC’s and Anabolic steroids; found in both men and women
Inflammatory hepatocellular adenomas, found in both men and women, and are associated with which disorder of the liver?
Risk of malignant transformation?
- NAFLD
- Small, but definitive risk of malignant transformation
Inflammatory hepatocellular adenomas are caused by activating mutations in what?
Leads to overexpression of?
gp130, a co-receptor for IL-6, that activates JAK-STAT signaling and overexpression of acute phase reactants
How do inflammatory hepatocellular adenomas differ in their morphology from the others?
Contain areas of fibrotic stroma + mononuclear inflammation + ductular rxns + dilated sinusoids, and telangiectatic vessels
Inflammatory hepatocellular adenomas often overexpress which acute phase reactants?
CRP and serum amyloid A
