Cervical and uterine Flashcards
What is the transformation zone in the cervix
- lies between exocervix and endocervical canal
- squamo-columnar junction
- metaplastic squamous epithelium

HPV 16 has a higher frequency of what type of cervical cancer
squamous cell carcinoma
HPV 18 has a higher frequency of what type of cervical cancer
adenocarcinoma
list the high risk and low risk strains of HPV
- high risk: 16, 18
- low risk: 6, 11
risk factors for HPV infection
multiple sex partners
What is the best screening test for cervical cancer
- HPV DNA testing
when is screening for cervical cancer initiated
- screen women starting at the age of 21 despite the age of sexual debut
- this recommendation does not apply to high-risk populations (immunocompromised)
what cervical cancer screening is done for women aged 21-29
- cytology performance only q 3 years
- DO NOT perfomr HPV DNA testing
what cervical cancer screening is done for women aged 30-64
- cytology + HPV DNA testing q 5 years or
- cytology alone q 3 years
who are the patients at high-risk for developing cervical cancer who need yearly screening
- HIV positive women
- immunocompromised
- personal hx of cervical cancer
- hx of CIN II/III
- exposure to DES in utero
When performing speculum examination and an abnormal cervical lesion is noted, perform what
-
biopsy
- not a pap smear
- a pap smear is a screening tool
- biopsy is diagnostic
- not a pap smear
follow up for women aged 21-24 who have atypical cells of undetermined significance (ASC-US)
- repeat pap smear in 1 year regardless of HPV result
follow up for women aged 24-64 who have atypical cells of undetermined significance (ASC-US)
-
must reflex to HPV DNA
- negative HPV DNA = normal cytology
- repeat pap smear/co-testing in 3 years
- positive HPV DNA -> refer for colposcopy
- negative HPV DNA = normal cytology
follow up for women aged 21-24 who have Low-grade squamous intraepithelial lesions (LSIL)
- repeat pap smear in 1 year regardless of HPV result
follow up for women aged 24-64 who have Low-grade squamous intraepithelial lesions (LSIL)
- refer for colposcopy despite HPV result or
- repeat Pap smear/co-testing in 1 yr if HPV DNA testing is negative
Low-grade squamous intraepithelial lesions (LSIL) are usually consistent with
- Cervical intraepithelial neoplasia I
follow up if “High-grade squamous intraepithelial lesion” (HSIL) is present
- assume HPV DNA is present
- refer for colposcopy (all ages)
“High-grade squamous intraepithelial lesion” (HSIL) are usually consistent with
- CIN II-III
followup for ages 21-29 with negative cytology, no endocervical cells
- routine screening - repeat Pap in 3 years
- DO NO perform HPV DNA testing
followup for ages > or = 30 with negative cytology, no endocervical cells
- perform HPV DNA testing
- negative: repeat pap in 5 years
- positive:
- refer for colposcopy if HPV 16/18 or
- repeat cytology and HPV in 12 months
differenatiate between cervical intraepithelial neoplasia I, II, and III
- I: involves lower third of epithelial lining
- II: involves lower two-thirds of epithelial lining
- III: involves more than two-thirds of epithial lining
What are the two types of cervical cancer
- cervical squamous cell cancer
- cervical adenocarcinoma
which HPV strains are most associated for cervical cancer
- HPV 16, 18
clinical presentation
- frequently asymptomatic
-
abnormal vaginal bleeding
- most common
- postcoital bleeding
- pelvic pain, unilateral with radiation into hip or thigh
- vaginal discharge
- cervical cancer
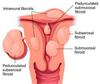
uterine fibroids arise from
smooth muscle cells within the uterine wall
where are submucosal uterine fibroids located
- lie just beneath the endometrium
where are subserosal uterine fibroids located
- lie just at the serosal surface of the uterus
where are intramural uterine fibroids located
- lie within the uterine wall
clinical presentation
- abnormal uterine bleeding
- pain
- pelvic pressure
- infertility
- spontaneous abortion
uterine fibroids
