Cardiovascular ( 20% ) Flashcards
- Muscarinic agonists may produce
- a. Mydriasis
- b. Vasodilatation
- c. Uterine contraction.
- d. Bronchodilatation
- e. B and C
e) B and C
(vasodilation + uterine contraction)
M3 contracts the pregnant uterus
M3 causes NO release from vascular endothelial cells->vasodilation
Mydriasis = anticholinergics (eg atropine)
Bronchodilation is caused by beta 2 stimulation
(Muscarinic agonists cause bronchoconstriction)
- Effects of isoprenaline include:
- a. Reflex bradycardia
- b. Decreased peripheral resistance.
- c. Marked hypertension
- d. Reduced pulse pressure
- e. A and C
b) decreasd PVR
Due to beta 2 stimulation causing vasodilation
Is also a positive inotrope and chronotrope->increased CO but also increase myocardial O2 demand
Increases pulse pressure by reducing diastolic BP and increasing systolic BP
Used in bradycardia and heart block
Beta agonist only -> vasodilation through beta-2 effects and baroreceptor response to increased cardiac output
- In the eye
- a. Alpha adrenoceptors cause contraction of the circular papillary muscle
- b. Cyclospasm is a feature of organophosphate poisoning
- c. Beta agonist will reduce intraocular pressure
- d. Antipsychotic agents such as chlorpromazine have no effect on the eye
- e. Diuretics have no use in glaucoma
b. Cyclospasm is a feature of organophosphate poisoning
Causes mydriasis (dilation) and cycloplegia
Beta blockers reduced IOP
- Which agonist is not correctly paired with its adrenoceptor?
- a. Phenylephrine – alpha 1
- b. Clonidine – alpha 2
- c. Dobutamine – beta 1
- d. Procaterol – beta 2
- e. Prazosin – alpha 2.
e. Prazosin
Is a alpha-1 selective antagonist
- Regarding beta-receptor antagonist drugs the following has no local anaesthetic action:
- a. Labetalol
- b. Atenolol
- c. Metoprolol
- d. Propranolol
- e. Pindolol
b) atenolol
Metoprolol, labetalol, propranolol do
Timolol, atenolol do not.
- regarding isoprenaline
- a. it is a potent bronchodilator
- b. it is a selective beta1 agonist.
- c. it can be used in tachyarrythmias to decrease AV conduction
- d. it has negative inotropic effects.
- e. it causes peripheral vasoconstriction
a) is a potent bronchodilator
Non-selective beta agonist
Positive inotrope and chronotrope
Causes peripheral vasodilation through B2 agonism
- regarding beta blockers
- a. inhibits renin release via beta2 receptors.
- b. metoprolol has intrinsic sympathomimetic effects.
- c. all are well absorbed
- d. beta1 selective antagonists don’t cause bronchoconstriction.
- e. can treat ventricular tachycardias
Nick thinks e) can treat ventricular tachycardias
Not sure about this - dont use betablockers for VT/VF or torsades etc, only for SVTs as they slow AV conduction.
I think it is C) all well absorbed
Inhibit renin release via beta 1 receptors
Celiprolol and labetalol have intrinsic sympathomimetic effects (ie partial agonism - avoids bradycardia, bronchospasm, and change in lipids)
beta 1 selective can still cause some bronchoconstriction
- IV drug that causes tachycardia, decreases diastolic BP, dilates pupil, doesn’t affect ejaculation, decreases sweating:
- a. Beta agonist
- b. Alpha antagonist
- c. Muscarinic antagonist
- d. Nicotinic antagonist.
- e. Nicotinic agonist
c. Muscarinic antagonist
Picture of anticholinergic syndrome
Tachycardia = Must be a beta agonist / parasympathetic antagonist
Reduces diastolic BP, dilates pupil (alpha antagonist or muscarinic antagonist)
Doesnt affect ejaculation, decreases sweating (not an alpha blocker / muscarinic antagonist)
Nicotinic antagonists dont affect ejaculation or dilate pupil
- Which has pure beta agonist effects in the circulation?
- a. Adrenaline
- b. Noradrenaline
- c. Isoprenaline
c. isoprenaline
A and NA both have alpha effects
- Choose the odd one out:
- a. Muscarine
- b. Acetylcholine
- c. Hyoscine.
- d. Bethanachol
c. Hyoscine.
Anticholinergic, others are cholinomimetics
- A young patient is given a normal dose of a drug in the emergency department. He develops tachycardia, increased BP and dilated pupils. The drug is most likely to be:
a. Adrenaline
b. Atropine.
b. Atropine.
Children notoriously sensitive to atropine but it has does not affect BP
- dobutamine
a. results in ATP -> AMP
b. can decrease systemic vascular resistance/afterload
b. can decrease systemic vascular resistance/afterload
Selective beta 1 agonist
Causes increased CO and decreased PVR
- regarding propranolol
- a. is a highly selective beta receptor antagonist
- b. is poorly lipid soluble
- c. has sodium channel blocking activity
c. has sodium channel blocking activity
Non-selective beta blockade
Lipophilic so it can cross the BBB
(and is thus used to treat anxiety and tremor)
- A young man presents with dilated pupils, confusion and hyperpyrexia. Which of the following could not account for these effects
- a. Atropine
- b. Datura
- c. Morphine
c. Morphine
Constricts pupils, does not cause hyperpyrexia
Datura and atropine are anticholinergics
‘Red as a beet, dry as a bone, blind as a bat, mad as a hatter’
- pralidoxime acts to
- a. inhibit presynaptic acetylcholine release
- b. cleave organophosphates from acetylcholinesterase
- c. regenerate acetylcholine
b. cleave organophosphates from acetylcholinesterase
Regenerates AChE in cases of organophosphate poisoning by removing the phosphate molecule that is blocking the receptor
- A patient comes in staggering, agitated and hyperthermic with dilated pupils. Which is LEAST likely to be the cause?
- a. Atropine overdose
- b. Amphetamines
- c. Angels trumpet
- d. Tricyclic overdose
- e. Aspirin overdose
e) aspirin OD
Aspirin blocks the krebs cycle->anaerobic metabolism-> lactic acidosis
Atropine + Angels trumpet - anticholinergic
Amphetamine - sympathomimetic
TCA - anticholinergic, indirect NA stimulation, alpha blockade
- benztropine causes:
- a. miosis
- b. diarrhoea
- c. confusion
- d. bronchorrhoea
- e. GIT haemorrhage
c. confusion
Benztropine = antimuscarinic
Drys secretions, hyperthermia, confusion, seizures, mydriasis, tachycardia, vasoconstriction, bronchial SM relaxing and reduced secretions.
- All of the following are characteristics of propranolol EXCEPT:
- a. Lipid soluble
- b. Local anaesthetic action
- c. Half life 3-6 hours
- d. Beta sympathetic selectivity
- e. 30% bioavailability
d. Beta sympathetic selectivity
Propranolol is a non-selective beta blocker
- regarding prazosin, which is NOT true?
- a. It is a selective alpha 1 blocker
- b. It dilates arterioles only, not veins
- c. It undergoes extensive first pass metabolism
- d. Recipients may develop a positive test for anti-nuclear factor
- e. With negative feedback of noradrenaline on its own, release can still occur
b. It dilates arterioles only, not veins
Alpha-1 specific blocker
relax arterial + venous smooth muscle, improve lipids, no reflex tachy, decrease afterload/preload(CHF)
All alpha-1 and beta blockers are well absorped but have high first pass metabolism
Phentolamine is a non-selective alpha blocker and causes a reduced TPR and a rebound tachycardia. Poor oral absorption.
- dopamine
- a. has less alpha agonist effect than dobutamine.
- b. dilates the renal vascular bed by its action of beta 1 receptors.
- c. causes a profound rise in peripheral vascular resistance
- d. is inactivated by sodium bicarbonate
- e. causes vasoconstriction at all doses.
d. is inactivated by sodium bicarbonate
(inactivated in akaline solution)
-
a. Dobutamine has alpha 1 and beta 1 activity. Dopamine also has alpha agonist activity
- Dopamine D1=D2>>B>>a
- Dobutamine B1>B2>>>>a
- b. dilates the renal vascular bed by its action of D1 receptors
- c. causes a rise in peripheral vascular resistance at high doses
- e. causes Vasodilation at lower doses but starts to act on alpha receptors at higher doses (alpha agonism -> vasoconstriction)
- propranolol
- a. has no central effects
- b. can be used safely in type I respiratory failure because of its reliable beta 1 selectivity
- c. in overdose may be effectively treated by administering glucagon
- d. needs to be given in relatively large oral doses because of its poor absorption
- e. does not produce withdrawal symptoms on abrupt cessation because beta receptors do not up regulate
c) Glucagon can be used in the OD of betablockers
- a) is lipophilic and crosses the BBB so has central effects (anxiety, tremor medication)
- b) Non-selective beta blockade, but even then you cannot safely use B1 selective agents in asthmatics.
- d) like all beta blockers is well-absorbed, but has high first pass metabolism
- e) beta receptors can upregulate
- hyoscine
- a. may potentiate the anticholinergic effects of phenothiazines
- b. is well absorbed from the gastrointestinal tract
- c. readily crosses the blood brain barrier
- d. has its main effect at nicotinic receptors.
- e. produces pronounced tachycardia in therapeutic doses
b) Atropine and Hyoscine are naturally-occuring alkaloid esters and are well absorped orally
- a. Phenothiazines do not appear to have much in the way of anticholinergic effects (do have extrapyamidal, sedative, and antihistamine/antinausea effects)
- c. hyoscine (used for nausea) does cross the BBB, hyoscine butylbromide (Buscopan) does not cross the BBB
- d. Has its effect at muscarinic receptors
- e. Can cause tachycardia in overdose
- beta blockers
- a. are class III antiarrythmic drugs.
- b. are selective for beta 1 adrenoreceptors.
- c. are useful agents in acute heart failure
- d. may mask the symptoms of hypoglycaemia
- e. are particularly safe and effective in combination with verapamil
d. may mask the symptoms of hypoglycaemia
(beta stimulation gives typical warning signs of tremor and palpitations etc)
- a. are Class II antiarrhythmics
- b. Can be beta-1 or non-selective
- c. Are dangerous in acute HF due to reduced inotropy
- e. have additive effects with verapamil and cause cariodepression
- atropine
- a. causes ureter and bladder wall contraction
- b. acts by blocking adrenoceptors
- c. is an example of a surmountable blockade
- d. results in miosis
- e. causes bradycardia in a moderate to high therapeutic dose
c. is an example of a surmountable blockade
- reversible blockade of muscarinic receptors and competitive antagonist of cholinomimetics*
- Causes ureter and bladder relaxation*
- Blocks muscarinic receptors*
- Causes mydriasis*
- Brady at low doses, tachy at high doses*
- noradrenaline
- a. is more potent than salbutamol at beta 1 receptors
- b. is less potent than isoprenaline at alpha receptors
- c. antagonizes the effects of dopamine
- d. has similar potency to adrenaline at beta 1 receptors
- e. is less potent than adrenaline at alpha receptors
d. has similar potency to adrenaline at beta 1 receptors
Norad: a1=a2; B1>>B2
Adrenaline: a1=a2; B1=B2
Isoprenaline B1=B2>>>>a
Salbutamol B2>B1
Is less potent than adrenaline at B2 receptors (hence why noradrenaline is a better pressor, as less vasodilation)
- which of the following drugs utilises camp as a second messenger?
- a. Adrenaline
- b. Dopamine
- c. Milrinone
- d. Glucagons
- e. All of the above
a) all of the above
Adrenergic and dopamine receptors are GPCRs
(D1 = Gs; D2 = Gi)
Milrinone inhibits Phosphodiesterase 3, which breaks down cAMP
Glucagon receptor has 3 subunits (a, B, y) and -> adenylyl cyclase -> cAMP
- which of the following statements is incorrect?
- a. Noradrenaline and adrenaline exert beta effects at low doses and alpha effects at high doses
- b. Dobutamine exerts its actions via alpha effects
- c. Inotropic agents act ultimately by increasing intracellular calcium
- d. Dopamine exerts different effects at different doses
- e. Theophylline is a positive inotrope
b. Dobutamine exerts its actions via beta effects
B1>B2>>>>a
Increase CO, reduce TPR
- milrinone
- a. has a short half life because of rapid reuptake and breakdown intravascularly by COMT
- b. is extensively metabolized by the liver.
- c. is in the same class of drugs as dobutamine
- d. is a competitive inhibitor of phosphodiesterase.
- e. is one of the most commonly used inotropes in the intensive care setting
d. is a competitive inhibitor of phosphodiesterase.
Prevents cAMP degradation
Has 12% liver metabolism
- alpha-adrenoceptors utilise
- a. camp as a second messenger
- b. cGMP as a second messenger
- c. phosphodiesterase inhibition to achieve positive inotropic effects
- d. phospholipase C to achieve positive inotropic effects
- e. a second messenger system that is yet to be discovered
d. phospholipase C to achieve positive inotropic effects
a1 -> Gq-> PLC -> IP3 + DAG -> Ca2+
a2 -> Gi ->reduce adenylyl cyclase->reduce cAMP
beta receptors utilise cAMP as a second messenger
Milrinone utilises phosphopdiesterase inhibition
- beta 1 effects include
- a. positive inotropy
- b. peripheral vasoconstriction
- c. bronchodilation
- d. peripheral vasodilation
- e. a and b only
a. positive inotropy
beta 2 causes skeletal muscle vasodilation
alpha causes skin and splanchnic vasoconstriction
B2 causes bronchodilation
- the following statements are true for catecholamines, EXCEPT:
- a. they all have a very short half life
- b. noradrenaline is used mainly when peripheral vasoconstriction is desirable
- c. dopamine in doses of <2mcg/kg/min has been proven to directly improve renal perfusion
- d. dobutamine is a synthetic derivative of isoprenaline
- e. they increase myocardial contractility at the expense of increased oxygen consumption
c. Despite improving renal blood flow, dopamine has not been shown to improve renal function in AKI
Dobutamine is a synthetic analogue of isoprenaline (which is itself synthetic)
All broken down rapidly by COMT and MAO
Norad causes more vasoconstriction than adrenaline and dopamine as it has less beta-2 agonism
. Digoxin
- a. Causes a decrease in intracellular sodium.
- b. Causes hypokalaemia in overdose.
- c. Has a half-life of 40 hours in a normal patient
- d. Decreases cardiac output.
- e. Has no role in the treatment of heart failure.
- a. Causes a increase in intracellular sodium
- b. Causes hyperkalaemia in overdose.
- c. Has a half-life of 40 hours in a normal patient
- d. increases cardiac output.
- e. Has a small and dated role in the treatment of heart failure.
- Digoxin
- a. Does not cross the blood brain barrier.
- b. Hypokalaemia decreases efficacy of digoxin.
- c. Hypomagnesaemia decreases efficacy of digoxin.
- d. Antibiotics have effects on digoxin.
- a. Does cross the blood brain barrier.
- b. Hypokalaemia increases efficacy of digoxin.
- c. Hypomagnesaemia increases efficacy of digoxin.
-
d. Antibiotics have effects on digoxin.
- Erythromycin inhibits PGP
- Digoxin
- a. Is not very lipid soluble and has a low volume of distribution.
- b. Is extensively metabolized prior to its excretion.
- c. Is highly protein bound.
- d. Has a half-life of 100 hours, thus allowing for once daily dosing.
- e. None of the above are correct
- a. Is lipid soluble and has a high volume of distribution.
- b. Is 33% metabolized prior to its excretion.
- Oral bioavailabilty and amount excreted unchanged in urine both 66%
- c. Is 25% protein bound.
- d. Has a half-life of 36 hours, thus allowing for once daily dosing.
- Steady state in 7 days
- e. None of the above are correct
- The electrical effects of digoxin in therapeutic concentrations include:
- a. The ability to revert atrial fibrillation to normal sinus rhythm in >60% of patients <12 hours
- b. No indirect effect (ie. Vagal) upon the Purkinje fibres in the ventricles.
- c. Increased refractory period at the atrioventricular node.
- d. Increased rate of firing of the sinoatrial node.
- e. ST segment elevation in the inferolateral segments of the ECG
- a. The ability to revert atrial fibrillation to normal sinus rhythm in >60% of patients <12 hours.
- Less effective and takes time
- b. Stimulates cholinergic transmission and has indirect effect (ie. Vagal) upon the Purkinje fibres in the ventricles, slowing conduction
-
c. Increased refractory period at the atrioventricular node.
- But reduces the RP in the atria, and also the AVN at toxic doses
- d. Decreased rate of firing of the sinoatrial node.
- e. ST segment elevation in the inferolateral segments of the ECG
- ?? likely not, havent seen this
Which of the following drugs has no significant interaction with digoxin?
- a. Quinidine.
- b. Amlodipine
- c. Verapamil.
- d. Warfarin.
- e. Thiazide diuretics.
- a. Quinidine.
- Increase plasma levels of digoxin by displacing tissue binding sites and depressing renal digoxin clearance
- b. Amlodipine
- c. Verapamil - Same as quinidine (as is amiodarone)
- d. Warfarin - 99% protein bound, so may displace digoxin
- e. Thiazide diuretics - Cause hypokalaemia -> increase toxicity risk
- Digoxin exerts its effects upon myocardial muscle at a cellular level by
- a. Increasing intracellular calcium
- b. Inducing Na+/K+/ATPase at the cell membrane
- c. Acting as a second messenger for G proteins
- d. Acting directly upon actin and myosin filaments to promote contractility
- a. Increasing intracellular calcium
- b. Inhibiting Na+/K+/ATPase at the cell membrane
- Digoxin Fab antibodies
- a. Are used routinely in the management of digoxin toxicity
- b. Decreases the serum digoxin level in the circulation
- c. Are commonly associated with tachyarrythmias after administration
- d. Take approximately 12 hours to have an effect
- e. Are metabolized in the liver
Nick has no answer
- a. Are used routinely in the management of digoxin toxicity
- Only if hypotensive/shocked, very high levels (eg >10ng/ml for acute ingestions), end-organ damage, symptomatic K+ >5.0
-
b. Decreases the serum digoxin level in the circulation
- Maybe? binds to digoxin, rendering it inert, then the complexes are renally excreted
- c. Are commonly associated with anaphylaxis to sheep protein after administration
- d. Take approximately 12 hours to have an effect
- Rapid onset effect I think
- e. Are metabolized in the liver
- Excreted in the kidneys
- The primary mechanism of action of digoxin involves:
- a. An increase in action potential amplitude
- b. An increase in ATP synthesis
- c. Modification of the actin molecule
- d. An increase in intracellular Ca2+ levels
- e. Block of the Na+/Ca2+ exchange
d. An increase in intracellular Ca2+ levels
- Regarding pharmacokinetics of digoxin
- a. It is poorly absorbed with oral administration.
- b. Its renal clearance is increased with renal disease.
- c. 40% of individuals have enteric bacteria inactivating it
- d. two thirds of digoxin is excreted by the kidneys
- e. the enterohepatic circulation contributes to the short half-life
- a. It is well-absorbed (66% bioavail) with oral administration.
- Reduced by antacids, increased by PPI
- b. Its renal clearance is decreased with renal disease.
- c. 40% of individuals have enteric bacteria inactivating it
- Dont think this is a thing
- d. two thirds of digoxin is excreted by the kidneys
- e. the enterohepatic circulation contributes to the short half-life
- t1/2 = 36 hours. Thats hardly short, is it?
- All of the following may increase the effect of digoxin EXCEPT:
- a. Amiodarone
- b. Frusemide.
- c. Carbamazepine
- d. verapamil
- e. quinidine
c. Carbamazepine
Amiodarone, verapamil, quinidine all increase plasma levels by displacing tissue binding sites and reducing renal excretion
Frusemide -> hypokalaemia, which increases the potential for ADRs
- Antiarrythmic drugs may work in any of the following ways EXCEPT:
- a. Reducing ectopic pacemaker activity
- b. Modifying conduction in re-entrant circuits
- c. Sodium channel blockade
- d. Calcium channel blockade
- e. Reducing the effective refractory period.
e. Reducing the effective refractory period.
They prolong the refractory period
Shortening it is pro-arrhythmogenic
Reduce ectopic activity- eg flecainide
Modify conduction - eg amiodarone
. Lignocaine
- a. Has poor oral bioavailability
- b. Blocks sodium channels not inactivated channels.
- c. Is effective in AF.
- d. Exacerbates VT in 30%
- e. Suppresses electrical activity of normal and arrythmogenic tissue equally.
a. Has poor oral bioavailability
- b. Blocks active and inactive sodium channels, not resting channels.
- c. Is ineffective in AF, due to less effect on atria. Hence Used for ventricular arrhythmias
- d. Exacerbates VT in 30%
- e. Affects arrhythmogenic tissue more (normal cells depolarise more often and clear the lidocaine)
. Flecainide
- a. Has poor oral bioavailability.
- b. Is safe in ischaemia induced arrhythmias.
- c. May be used in reentry tachycardias
- d. Is a class Ia antiarrythmic.
- e. Reduces mortality in post MI PVCs.
- a. Has good oral bioavailability - so can use as ‘pill in the pocket’ for SVT
- b. Is fuckin dangerous in ischaemia induced arrhythmias, and will muder you if you have had an MI in the past or a structurally abnormal heart
-
c. May be used in reentry tachycardias
- eg SVT, AVNRT
- d. Is a class Ic antiarrythmic.
- Ia is procainamide, TCAs, quinidine
- e. Increases mortality in post MI PVCs (see note above re murder)
- adenosine
- a. has a half life of 2 minutes.
- b. increases AV nodal conduction.
- c. predominantly inhibits sinoatrial nodal function.
- d. directly inhibits AV nodal conduction
- e. is more effective in the presence of theophylline or caffeine
- a. has a half life of 10 seconds
- b. Slows/stops AV nodal conduction
- c. predominantly inhibits Atrioventricular nodal function (AVN>SAN)
-
d. directly inhibits AV nodal conduction
- By opening K+ channels -> hyperpolarising the cells and preventing them depolarising
- e. is less effective in the presence of theophylline or caffeine.
- adenosine
- a. has a half life of 30 seconds.
- b. is the drug of choice for ventricular tachyarrythmias.
- c. works by directly inhibiting the sinoatrial node with only mild effect on the atrioventricular node.
- d. causes flushing in over 50% of patients.
- e. is less effective in the presence of caffeine and theophylline
- a. has a half life of 10 seconds
- b. is the drug of choice for atrial tachyarrythmias
- Blocks AV node, hence reduces the rate of impulses propogated, allowing atria time to reset
- c. works by directly inhibiting the atrioventricular node with only mild effect on the sinoatrial node.
- d. causes flushing in 20% of patients.
- e. is less effective in the presence of caffeine and theophylline
- regarding antiarrythmics
- a. adenosine alters QRS duration
- b. amiodarone has a short half life
- c. lignocaine is also useful in supraventricular arrythmias
- d. flecainide is unsafe in people with ischaemic heart disease
- e. quinidine has no effect on QRS duration
- a. adenosine alters QRS duration - wrong. Prevents AV conduction by hyperpolarising the cell
- b. amiodarone has a fucking long half life - 58 days!
- c. lignocaine is also useful in supraventricular arrythmias
- Greater effect on ventricles than atria - good for VT/VF
-
d. flecainide is unsafe in people with ischaemic heart disease
- Risk of developing VT
- e. quinidine has no effect on QRS duration
- Class Ia, so prolongs the AP -> slowed conduction -> wide QRS
- amiodarone
- a. is only effective in suppression of ventricular arrythmias
- b. causes peripheral vasodilation via alpha-adrenergic effects
- c. commonly causes corneal opacification
- d. increases warfarin clearance
- e. decreases AV nodal refractory period
- a. is only effective in suppression of ventricular arrythmias
- Wrong - can use for AF
- b. causes peripheral vasodilation via alpha-adrenergic effects
- c. commonly causes pulmonary fibrosis
- d. Decreases warfarin clearance
- As well as statins and digoxin
- e. increases AV nodal refractory period (can cause AV nodal block)
- lignocaine displays all of the following EXCEPT:
- a. increased action potential duration
- b. binding to both activated and inactivated sodium channels
- c. predominant metabolism
- d. decreased clearance associated with concomitant propranolol administration
- e. ineffectiveness against arrhythmias in normally polarize tissues
Lignocaine is a Class Ib antiarrhythmic
Therefore it Shortens AP duration with a weak Na block
a. increased action potential duration
- which of the following does NOT prolong the effective refractory period in the atrioventricular node?
- a. Propranolol
- b. Amiodarone
- c. Flecainide
- d. Verapamil
- e. Phenytoin
c. Flecainide
Class 1c - normal ERP and AP duration

- adenosine
- a. is effective in converting atrial flutter
- b. depresses conduction through the AV node
- c. requires reduction of dose in patients with hepatic failure
- d. has a half life of 30-60 seconds
- e. is safe in sick sinus syndrome
b. depresses conduction through the AV node
- amiodarone
- a. has a short half life.
- b. stimulates Na channels.
- c. is only effective against ventricular arrhythmias.
- d. has antianginal effects.
- e. can cause emphysema in 5-15% of people.
- a. has a looooong half life - like, 1 week
- b. Blocks Na channels - Class I activity
- c. is effective against both atrial and ventricular arrhythmias.
- d. has antianginal effects - Due to calcium and beta-blocking activity (class IV and II)
- e. can cause pulmonary fibrosis around 1% of patients
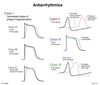
- In the Vaughan-Williams classification
- a. Class 1 drugs affect potassium channels
- b. Class II drugs affect calcium channels
- c. Class II drugs affect sodium channels
- d. Class III drugs affect potassium channels
- e. Class IV drugs affect chloride channels
- a. Class 1 drugs affect sodium channels
- b. Class II drugs affect beta receptors
- c. Class II drugs affect beta receptors
- d. Class III drugs affect potassium channels
- e. Class IV drugs affect calcium channels
- In therapeutic doses, adenosine:
- a. Acts by affecting sodium channels
- b. Is administered as a slow IV push.
- c. Is metabolized in the liver
- d. Produces a bradycardia by vagal stimulation
- e. Affects adenosine receptors at the AV node
e. Affects adenosine receptors at the AV node
- adenosine
- a. opens K+ channels
- b. opens Cl- channels
- c. half life of 10min
- d. profoundly blocks SA node
- e. blocks Ca2+ dependent action potential
a. opens K+ channels
- regarding adenosine
- a. its receptors are ion channels
- b. it increases AV nodal conduction
- c. it enhances K+ conductance
- d. it is the drug of choice in VF
- e. it has a half life of 2 minutes
c. it enhances K+ conductance
Receptor is a GPCR with caffeine and theophylline as antagonists
- which doesn’t prolong the refractory period in normal cells?
- a. Amiodarone
- b. Lignocaine
- c. Sotalol
- d. Quinine
- e. Procainamide
b. Lignocaine
Shortens it as a class Ib
Class Ic has no effect
Class II has no effect.
All others prolong
- regarding amiodarone
- a. it has no alpha adrenergic effects
- b. it has no beta adrenergic effects
- c. it has low affinity for activated sodium channels
- d. it increases warfarin clearance
- e. it enhances conduction through accessory pathways
c. it has low affinity for activated sodium channels
Has class I, II, III, IV activity
But only acts on inactivated Na channels
Reduces warfarin metabolism -> increased effect
- amiodarone
- a. has a low affinity for activated sodium channels
- b. is associated with thyroid dysfunction in 50% of patients
- c. has a half-life of 8-20 days
- d. increases clearance of warfarin
- e. commonly causes peripheral vasoconstriction
-
a. has a low affinity for activated sodium channels
- Works only on inactivated channels
- b. is associated with thyroid dysfunction in 50% of patients
- c. has a half-life of 56 days!!!
- d. decreases metabolism of warfarin
- e. occasionally causes peripheral vasodilation due to alpha blockade
- which does not prolong the refractory period of normal cells
- a. amiodarone
- b. lignocaine
- c. quinidine
- d. sotalol
- e. procainamide
b. lignocaine
Class Ib - shortens (lidocaine, phenyotoin)
Class Ic - no effect (flecainide)
Class II (beta blockers) - no effect
Others all prolong
- the most common adverse effect of procainamide is
- a. bradycardia
- b. pulmonary infiltrates
- c. fever
- d. hypotension
- e. anaphylaxis
d. hypotension
Can also cause QT prolongation -> torsades, or a lupus-like effect (as does hydralazine) which spares the kidneys, and resolves with stopping the medication
- mannitol
- a. inhibits H20 absorption in proximal tubule, loop of Henle and collecting tubule
- b. is metabolized to glycerol
- c. decreases total body water and total body cation content equally.
- d. is of no value when renal haemodynamics are compromised.
d. is of no value when renal haemodynamics are compromised.
As it requires filtration, which wont happen if renal blood flow is compromised. This can lead to oedema and hyponatraemia (contraindicated in anuria)
a. inhibits H20 absorption in proximal tubule and loop of Henle, but not the collecting duct
Nick says A is right however I cannot find anywhere that lists CD as a site of action of mannitol in addition to PCT/LoH. d) would seem to be the more correct answer.
- b. is not metabolised
- c. decreases total body water more than total body cation content equally (hence can cause hypernatraemia)
- which raises the pH of urine the most
- a. acetazolamide
- b. frusemide.
- c. chlorthiazide.
a. acetazolamide
creates urinary alkilisation
Other agents cause H+ loss and so acidify the urine
- which is NOT true of diuretics?
- a. Loop diuretics can be used to treat hypercalcaemia
- b. Frusemide is used in the prophylaxis of acute mountain sickness.
- c. Cirrhotic oedema responds to spironolactone
- d. They may enhance the efficiency of ACE inhibitors
- e. Hydrochlorothiazide is useful in diabetes insipidus
b. Acetazolamide is used in the prophylaxis of acute mountain sickness.
a) frusemide inhibits Na-2CL-K symporter. Due to the potential changes by impacting K+, less Mg and Ca is reabsorbed.
- Which is the correct site of action?
- a. Spironolactone = collecting duct.
- b. Triamterene = ascending loop of Henle
- c. Thiazides = proximal part of distal tubule.
- d. Frusemide = proximal tubule
- e. Acetazolamide = collecting tubule
a. Spironolactone = collecting duct.
c. Thiazides = distal tubule (Na-Cl symporter)
Cannot find which part of the DCT is the site of action for thiazides, so i think a) is the more correct answer.
- b. Triamterene = Blocks ENaC in CD (potassium sparing diuretic)
- d. Frusemide = ascending limb of thick LoH (Na-2Cl-K symporter)
- e. Acetazolamide = PCT (Carbonic anhydrase)
- Loop diuretics (eg frusemide) inhibit:
- a. Na+/Cl- channels
- b. K+/H2CO3 channels
- c. Na+/K+/2Cl- channels
- d. Na+/glucose symporter
- e. Na+/K+ channels
c. Na+/K+/2Cl- channels
- In the thick part of ascending LoH*
- Thiazides inhibit Na-Cl*
- Spironolactone inhibits basal Na-K channels*
- The elimination half-life of frusemide is:
- a. 30min – 1hr
- b. 1-2hr
- c. 1.5-2hr
- d. 2-3hr
- e. 2.5-3hr
c. 1.5-2hr
- Which of the following is an aldosterone antagonist?
* d. spironolactone - An example of an ADH antagonist is
- a. Ethanol
- b. Amiloride
- c. Lithium
- d. Aldosterone
- e. Triamterene
c. Lithium
a. Ethanol
* Nick says Lithium (this enters the principal cells and interferes with aquaporin function, causing ADH resistance). This is probably correct*
* Ethanol and water both inhibit ADH secretion.*
- Carbonic anhydrase inhibitors
- a. Were developed from early antibiotics
- b. Are closely related to thiazide diuretics
- c. Cause metabolic acidosis
- d. Decrease the pH of CSF
- e. All of the above
e. All of the above
- Which is not the correct site of action
- a. Spironolactone and the collecting duct
- b. Triamterene and the collecting duct
- c. Thiazides and the proximal part of the distal tubule
- d. Acetazolamide and the collecting tubule
- e. Frusemide and the ascending loop of Henle
d. Acetazolamide and the PCT
Triamterene is a potassium-sparing diuretic which directly blocks ENaCs in the CD -> reduced Na reabsorption -> diuresis
