Cardiology Flashcards
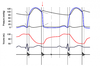
The above are electrocardiogram recordings (paper speed = 25mm/s) from the same horse taken at different time points during the same 24 hour interval. Which of the following horses is most likely to belong to the above electrocardiogram recordings?
A. 4 year old Thoroughbred mare in race training in California who galloped today.
B. 8 year old Arabian stallion who has just completed an 80km endurance ride.
C. 12 year old Quarter Horse gelding undergoing general anaesthesia for a cryptorchid castration.
D. 2 day old Lusitano filly foal with clostridial diarrhoea.

C. 12 year old American Quarter Horse gelding undergoing general anaesthesia for a cryptorchid castration.
Findings on the ECG are consistent with hyperkalaemia i.e. decreased amplitude and prolonged duration of P waves and increased amplitude of T waves (not yet bradycardic, but HR did decrease from 46bpm when normokalaemic to 35bpm). The American Quarter Horse in question was heterozygous for HYPP and an acute episode of HYPP was triggered by anaesthesia.
Ref: Carpenter and Evans, JAVMA, 2005; 226:874-876.
You collect electrocardiogram readings (paper speed = 25mm/s, gain = 10mm/mV) from endurance horses during the final veterinary inspection of a 120km endurance ride as part of a research project. You identify the above abnormality on a horse that successfully completed the ride. What do you advise the owner regarding this result?
A. The two arrows highlight supraventricular premature complexes. It is not normal to identify these following endurance exercise, therefore the horse likely has an unrelated myocardial disorder which should be investigated before it is next ridden.
B. The two arrows highlight supraventricular premature complexes. These are frequently observed in endurance horses following long rides who appear to be otherwise healthy.
C. The two arrows highlight ventricular premature complexes. It is not normal to identify these following endurance exercise, therefore the horse likely has an unrelated myocardial disorder which should be investigated before it is next ridden.
D. The two arrows highlight ventricular premature complexes. These are frequently observed in endurance horses following long rides who appear to be otherwise healthy.

D. The two arrows highlight ventricular premature complexes. These are frequently observed in endurance horses following long rides who appear to be otherwise healthy.
Ref: Flethoj et al, JAVMA 2016; 248:1034-1032.
Your client calls you very excited as she thinks she has found the perfect new horse! It is an 8 year old Holsteiner gelding that is training Prix St George dressage. The local vet called her while performing the pre-purchase examination and said the horse’s general body condition, brief lameness examination and ocular examination findings were within normal limits, but that he would recommended an electrocardiogram (paper speed = 25mm/s, gain = 10mm/mV). She shows you the trace he sent her and asks you to explain its significant to her. You tell her:
A. This ECG shows a normal heart rate and rhythm with the shaky line just due to movement artifacts, and if the remainder of his physical examination findings are within normal limits, does not provide evidence the horse should fail the pre-purchase examination.
B. This ECG shows ventricular tachycardia, which is a potentially life-limiting condition, and you could not recommend the purchase the horse without further cardiac evaluation being performed.
C. This ECG shows atrial tachycardia, which is a potentially life-limiting condition, and you could not recommend the purchase the horse without further cardiac evaluation being performed.
D. This ECG shows atrial fibrillation, and further examination of the horse by a veterinary cardiologist or equine medicine specialist is recommended prior to considering purchase of this horse.

D. This ECG shows atrial fibrillation, and further examination of the horse by a veterinary cardiologist or equine medicine specialist is recommended prior to considering purchase of this horse.
NB This was a tricky one!! It is AFib, as evident by the coarse f waves and lack of P waves BUT the R-R interval is regular (‘regularised AF’)…this is because none of the atrial impulses are conducted to the ventricles, i.e. complete heart block is present, and the narrow QRSs are a junctional escape rhythm (coming from the AV junction).
ECG from: http://lifeinthefastlane.com/ecg-library/junctional-escape-rhythm/
Above is an electrocardiogram trace (paper speed = 25mm/s, gain = 5mm/mV) from a 19 year old Australian Stock Horse used for campdrafting that presented to your clinic for evaluation of poor performance. Correctly identify the arrhythmia shown on the trace and its cause.
A. First degree atrioventricular block; high vagal tone.
B. Second degree atrioventricular block, Mobitz type I; high vagal tone.
C. High degree/advanced second degree atrioventricular block; digitalis toxicity.
D. Third degree/complete atrioventricular block; myocarditis.

C. High degree/advanced second degree atrioventricular block; digitalis toxicity.
1st degree AV block is characterised by prolonged PR interval but there is a QRS for every P.
2nd degree AV block is characterised by regular P waves but intermittent missed QRS complexes; consecutive QRS complexes are not missed; in Mobitz I (Wenckebach, physiologic) there is progressive prolongation of the PQ interval before the dropped QRS, in Mobitz II (pathologic) there is no prolongation of the PQ interval.
High degree/advanced AV block is characterised by regular P waves with a run of consecutive missed QRS complexes; there may or may not be prolongation of the PQ interval; this is pathologic (AV nodal dz, digitalis, electrolyte) and the horse may exhibit severe exercise intolerance and syncope.
3rd degree AV block is complete lack of AV conduction i.e. regular P waves from the SA node with occasional wide bizarre QRS of idionodal or idioventricular origin; pathologic with severe AV nodal dz e.g. lymphoma, rattlesnake envenomation.
Ref: http://veteriankey.com/dysrhythmias-assessment-and-medical-management/
Which of the following images below shows a ventricular premature depolarisation?

A. This is a VPC as it is a wide and bizarre QRS complex without a preceding P wave.
B and C are examples of bundle branch block – they also have a wide and bizarre QRS complex, but there is a preceding P wave.
D is a supraventricular (atrial) premature complex – there is an abnormally shaped, early P wave (can sometimes occur with previous T wave) before a normal (narrow) QRS complex.
You perform a physical examination on a very nervous horse 2 minutes after it is unloaded from a horse truck at an international level showjumping competition in accordance with the quarantine rules of the event. It is breathing irregularly and snorting at shadows and you hear what you suspect is a sinus arrhythmia. You perform an electrocardiogram to further assess the arrhythmia, as shown above. What do you advise the person responsible for the horse?
A. The arrows indicate atrial premature complexes, which are not significant in terms of performance if they only occur occasionally, but can increase the risk of developing atrial fibrillation in the future.
B. The arrows indicate supraventricular premature complexes which indicate cardiac pathology if they occur at a rate of more than 2 per minute, therefore this horse should have an exercising ECG performed before it is allowed to compete.
C. The horse has a wandering pacemaker. This is not significant in this case as all other beats are in sinus rhythm, indicating normal sinoatrial and atrioventricular conduction.
D. The horse has a sinus arrhythmia in which the heart rate varies in concert with changes in the respiratory rate and is of no clinical significance.

A. The arrows indicate atrial premature complexes, which are not significant in terms of performance if they only occur occasionally, but can increase the risk of developing atrial fibrillation in the future.
It would probably be a good idea to do an exercising ECG to make sure that the APCs disappear or remain very occasional as there are 2 in a single trace here! The actual trace is from a foal that was bitten by a snake and was in DIC and they resolved 6wks post-presentation to hospital.
Ref: Colour Atlas of Diseases and Disorders of the Foal pg 206.
What is the recommended treatment for a horse with the following electrocardiogram recording:
A. Quinidine administered via nasogastric tube.
B. Intravenous digoxin.
C. Intravenous lidocaine.
D. Oral amlodipine.

C. Intravenous lidocaine – class 1b anti-arrhythmic which blocks the rapid Na channel.
The ECG shows ventricular tachycardia – HR = ~200bpm, complete dissociation of P and QRS.
Quinidine is for atrial fibrillation.
Digoxin has indirect anti-arrhythmic effects by increasing vagal tone and decreasing sympathetic tone; it is used to decrease ventricular response rate in atrial fibrillation.
Amlodipine is an angioselective calcium channel blocker used in treatment of hypertension.
ECG from Colour Atlas of Diseases and Disorders of the Foal pg 206.
What is represented by the red arrow in the following diagram of the cardiac cycle?
A. Rapid inflow.
B. Isovolumic relaxation.
C. Atrial systole.
D. Atrioventricular valves opening.
B. Isovolumic relaxation.
What does S4 represent?
A. Mitral and tricuspid valve closure.
B. Pulmonic and aortic valve closure.
C. Atrial contraction.
D. Ventricular filling.
C. Atrial contraction.
S1: associated with closure of the AV (M and T) valves and turbulence in large vessels during early systole. Usually louder, longer and lower pitched than S2 with PMI over the left apex. Split S1 may be normal.
S2: associated with closure of the A and P valves. Usually sharper, shorter and higher pitched than S1 with PMI over the heart base. Split S2 may be normal or associated with cardiac disease.
S3: associated with rapid ventricular filling early during diastole. Usually heard immediately after S2 with PMI over the left apex.
associated with atrial contraction at the end of diastole. Usually heard immediately before S1 with PMI over the left base.
Which of the following is a feature of cardiac muscle but is not a feature of skeletal muscle?
A. The muscle action potential depends on the opening of fast sodium channels.
B. Intercalated disks between myocytes allow cells to fuse together to form gap junctions, which in turn allow ions to diffuse freely from cell to cell.
C. Actin and myosin binding is regulated by the tropomyosin-troponin system.
D. Myocytes are multinucleated.
B. Intercalated disks between myocytes allow cells to fuse together to form gap junctions, which in turn allow ions to diffuse freely from cell to cell.
Both skeletal and cardiac muscle APs rely on fast Na channels, but cardiac muscle Aps also rely on slow Ca channels.
The tropomycin-troponin system regulates actin and myosin binding in both types of muscle.
Skeletal muscle myocytes are multinucleated, whereas cardiac myocytes general only have one nucleus.
What is the result of acetylcholine release on the heart?
A. Decreased rate of sinus nodal rhythm and decreased excitability of atrioventricular junctional fibres.
B. Increased cardiac myocyte permeability to sodium and calcium.
C. Decreased cardiac myocyte permeability to potassium.
D. Decreased rate of sinus nodal rhythm and increased excitability of atrioventricular junctional fibres.
A. Decreased rate of sinus nodal rhythm and decreased excitability of atrioventricular junctional fibres.
Increased parasympathetic (vagal) tone è acetylcholine release à increased permeability of cardiac myocytes to potassium and decreased permeability to sodium and potassium à decreased SA node rate and AV excitability.
NB Parasympathetic nerve fibres are distributed mostly to the atria…that’s why heart rate is effected more dramatically than strength of contraction (vs sympathetic stimulation à increased heart rate and force of contraction).
Select the option below in which the protein and its action are correctly paired:
A. Troponin C; inhibits actin-myosin binding.
B. Tropomyosin; winds around myosin to cover the actin binding sites.
C. Troponin I; binds to calcium to inactivate troponin C and therefore promotes actin-myosin binding.
D. Troponin T; binds the troponin-tropomyosin complex to the actin filament.
D. Troponin T; binds the troponin-tropomyosin complex to the actin filament.
Tropomyosin winds around actin, hides the myosin biding sites.
Troponin I inhibits actin-myosin binding.
Troponin C binds intracellular Ca++.
When Ca++ binds to troponin C, the inhibitory action of troponin I is ‘shut off’, the troponin-tropomyosin complex shifts and actin-myosin binding occurs.
Which of the following is an indication for quinidine cardioversion in an eight year old Warmblood mare used for eventing with atrial fibrillation?
A. Marked atrial enlargement.
B. Complex ventricular ectopy.
C. Lone atrial fibrillation.
D. Marked valvular degeneration.
C. Lone atrial fibrillation.
Ref: ACVIM/ECEIM consensus statement 2013: Recommendations for Equine Athletes with Cardiovascular Abnormalities.
Which of the following could be considered a common cause of tricuspid regurgitation?
A. Regurgitation secondary to severe respiratory disease.
B. Congenital tricuspid valve abnormalities.
C. Valvular endocarditis.
D. Training-associated regurgitation in high-level athletes.
D. Training-associated regurgitation in high-level athletes.
Ref: ACVIM/ECEIM consensus statement 2013: Recommendations for Equine Athletes with Cardiovascular Abnormalities.
Horses in elite competition undergo frequent management changes due to their competition schedule. Ohmura et al, AJVR 2012, investigated the effects of transport and fasting on cardiac parameters in healthy Thoroughbreds and Warmbloods. Which statement is most consistent with their findings?
A. Heart rate variability indices are influenced by transport and fasting in a manner consistent with alterations in sympathovagal balance induced by these management changes.
B. Fasting influences the circadian rhythm of the heart, such that peak heart rate occurs from 6am to 8am in horses followed a 24-hour fast, as opposed to fed horses in which peak heart rate occurs at 7-8pm.
C. Second degree atrioventricular block is more common in horses that are undergoing stall rest than in those undergoing air transportation.
D. Air transport and fasting exert a greater influence on the ratio of low frequency:high frequency heart rate variability than road transport in horses.
A. Heart rate variability indices are influenced by transport and fasting in a manner consistent with alterations in sympathovagal balance induced by these management changes.
Fasting increased parasympathetic tone à more frequent AV block, higher low frequency and high frequency heart rate variability.
Transport à stress à increased sympathetic tone à increased heart rate, no influence on high frequency heart rate variability indices but some influence on low frequency heart rate variability.
B. Fasting did not alter the circadian rhythm of the heart rate; higher HR still occur at 7-8pm.
C. This is quite possibly true, but they did not record arrhythmias in the transport group.
D. Fasting significantly influenced the LF:HF heart rate variability ratio but transport did not.
Ref: Ohmura et al, AJVR 2012; 73:508-514 and Ohmura et al, AJVR 2012; 73:515-521.