Burns Flashcards
Incidence statistics for burns?
- 1.25 million burns annually worldwide
- 486,000/year in US required ER visits
- 40,000 hospitalized
- 30,000 admitted to specialized burn center
- incidence of burns has decreased secondary to education on prevention and safety regulations
- survival rate 96.8%
Where they occur
- 73% home
- 8% occupational
- 5% traffic accidence
- 5% recreational sport
- 9% other causes
Etiology of burns?
- Electricla burn 4%
- Chemical burn 3%
- Inhalational burn (burn in a closed space is suspicious for inhalational)
- no percent on chart
- Thermal burn 43%
- (same as flame/fire on pie chart provided)
Mortality of burns?
-
INCREASED MORTALITY
- Older age >60 yo
- >40% TBSA
- inhalational injury
- age of patient + %TBSA burned if > 115, then mortality of patient >80%
- mortality doubled if burn + inhalational injury
- Burn size with LD 50 *lethal dose 50%* >90% TBSA (total body surface area)
- Approx. 3240 die from fire/smoke inhalation injury
- 2855 from residential fires
- 300 motor vehicle/aircraft
- 75% dies at scene or during transport
- 35% burn victims <17 yo
-
Decreased mortality in burns due to:
- increased access emergenyc care
- better airway mgmt
- better infection contorl
- better nutritional support
- early burn excision/grafting
- treatment of hypermetabolic response with EBP
*
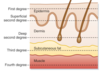
Anatomy of integumentary system
- Largest organ
- layers
- epidermis- protective outer surface
- avascular. nourished by dermis
- dermis
- vascular
- heavily innervated
- collagen and elastic fibers
- deep layer dermis- hair follicles, sebaceous gland. afferent nerve endings
- most nerve terminals at dermis and a few penetrate the epidermis
- deep fascia- deepest layer, dense organized connective tissue layer, seats skin into sq tissue
- subcutaneous
- epidermis- protective outer surface
Function
- protection
- immune function
- fluid/electrolyte homeostasis
- containment
- heat regulation
- sweating/vasomotor regulation of superficial blood flow
- blood vessels dilate in heat, constrict in cold
- sweating/vasomotor regulation of superficial blood flow
- sensation
- vitamin D

Burn categorization?
- Basis: depth and body surface area
- 1st degree- epidermis
- heals spontaneously
- 2nd degree- important to know if basement membrane is intact/not intact
- superficial partial thickness (basement membrane intact)
- if basement membrane intact- skin will generate and grafting not needed
- deep dermal burn (basement membrane not intact)
- need grafting
- superficial partial thickness (basement membrane intact)
- 3rd degree- full thickness burns
- subcutaneous extension
- will need grafting
- 4th degree
- muscle, fascia, bone

What is a first degree burn?
depth? how the wound looks? causes? levelof pain? healing time? scarring?
- Depth- epithelium
- How the wound looks- no blisters; dry, pink
- Causes- sunburn, scald, flash flame
- Level of pain- painful, tender and sore
- Healing time- two to five days; peeling
- Scarring- no scarring, may have discoloration
What is a second degree burn?
depth? how the wound looks? causes? level of pain? healing time? scarring?
- Depth- epithelium and top aspect of dermis
- How it looks- moist, oozing, blisters,
- moist, white, pink to red
- Causes
- scalds
- flash burns
- chemicals
- Level of pain
- very painful
- Healing time
- superficial- five to 21 days- no grafting needed
- deep 21-35 days- needs grafting
- Scarring
- minimal to no scarring
- may have discoloration
Characteristics of third degree burn?
depth? how the wound looks? causes? level of pain? healing time? scarring?
aka full thickness
- Depth- epithelium and dermis
- how it looks-
- leathery, dry
- no elasticity
- charred
- Causes
- contact with flame, hot surface
- hot liquids
- chemical
- electrical
- Level fo pain
- very little pain or no pain
- Healing time
- small areas may take months to heal
- large areas to be grafted
- Scarring present
Summary of burns?
- 1st degree
- involves epidermis
- erythema
- spontaneous healing
- 2nd degree
- superficial burn
- spontaneous healing 7-10 days
- painful
- deep dermal
- requires excision/grafting
- 2-8 weeks to heal
- scarring
- superficial burn
- 3rd degree- complete dermal loss
- no pain d/t nerve damage
- 4th degree- expect to lose limb
- muscle/bone/tnedon involved
What is the rule of nines?
- How we estimate burns
- Head and neck 9% (total)
- Ant 4.5%
- Post 4.5%
- RUE 9%
- Ant 4.5%
- Post 4.5%
- LUE 9%
- Ant 4.5%
- Post 4.5%
- RLE 18%
- Ant- 9%
- Post 9%
- LLE 18%
- Ant- 9%
- Post 9%
- Anterior tunk 18%
- Post trunk 18%
- Perineum 1%

Criteria of major burn?
2nd degree burn >20% TBSA in adult, or 10% in extremes of age
or
3rd degree burn >10% TBSA in adult
or
any electrical burn
or
any burn associated with smoke inhalational
or
any burn involving face, airway, or genitals of any percent
What determines initial resuscitation in burn
TBSA
How is TBSA estimated in children?
- Lund and Browder chart
- not expected to memorize
- Rules of nine inaccurate in children
- head and trunk proportionally larger in children
Pathophysiology of burns?
- 2 distinct phases
- burn/shock phase
- hypermetabolic phase
- SIRS response
- every system affected
- necrotic and ischemic area
- potential viability of ischemic area with adequate resuscitation
- no potential for viability with necrotic area
- Minutes to hours: burned tissues release inflammatory and vasocative mediators
- All lead to increased capillary permeability,
- histamine
- prostaglandin
- kinin
- leukotrienese
- thomboxane
- nitric oxide
- All lead to increased capillary permeability,
- Later
- reperfusion injury
- tissue produces ROS and toxic cell metabolites
- leads to further cell membrane dysfunction
- worsening of immune response, cascade of responses
- reperfusion injury
What should we keep in mind in regards to burn zones?
- Burn
- zone of coagulation- area dead
- zone of stasis
- zone of hyperemia
- with adequate resuscitation, zone of stasis and zone of hyperemia blood flow can be restored and maintain viabiilty
- without adequate resus, the zone of coagulation will grow and zone of stasis will become infarcted and won’t be able to regenerate

Electrical burns?
- Devastating injury to bones, BV, muscle, and nerves
- tissue damage based on voltage and duration
- entry and exit are where most energy (damage) are concentrated
- 10-46% with concurrent cardiac arrhythmias; may have damage to the myocardium
- massive muscle damage leads to renal failure secondary to myoglobinemia (from rhabdo)
Chemical burns?
- Occupational injury
- reaction with tissue proteins and cellular components leads to tissue destruction
- chemical burn: must neutralize; copious irrigation
Thermal burns?
- Scaled inuries account for 70% burns in <4 yo
- >5 yo: flame associated
- burns in young children 15-20% is non-acciedental burn (d/t abuse/neglect)
Symptoms Inhalational injury?
- hoarseness
- sore throat
- dysphagia
- hemoptysis
- tachypnea
- accessory muscle usage
- wheezing
- carbonaceous sputum
- increased CO levles
Types of inhalational burns?
- Most commonly associated with thermal burns
- likely in closed space burn; suspect in pt unconscious at scene
3 types
- 1) Upper airway injuries- inhalation of superheated air/steam
- may spare lower airway d/t reflexive VC closure
- 2) Lower airway/parenchymal
- soot particle/chemical inhalation
- acute phase will have significant bronchopasms
- bronchodilator therapy always required
- may need epi b/c refractory to other treatment
- bronchodilator therapy always required
- 3) metabolic asphyxiation- carbon monoxide, etc.
Pathophys of inhalational injury?
- microvascular changes
- heat denatures proteins, activates complements
- causes release of histamine
- histamine causes release of xanthin oxidase
- enzyme involved in breakdown of purine–> uric acid
- ROS released
- ROS combine with NO–> reactive nitrogen species formed
- causes edema in burned area
- increases microvascular pressure and permeability to protein
- ROS combine with NO–> reactive nitrogen species formed
- release proinflammatory cytokine and oxygen free radical/interleukin
- attract polymorphonuclear cells to area and neutrophils applify release of oxygen radicals, proteases and other materials
- becomes vicious cycle

Consequence of inhalational injury?
- Coagulopathy
- Bronchospasm
- mucus secretion–> airway obstruction
- airway epithelial exfoliation because of neutrophil migration
- increased airway blood flow
- causes airway wall edema
- upregulation of adhesion molecules, ROS, superoxide
- end up with lots of cellular dysfunction, pulmonary edema, V/Q mismatch, loss of hypoxic vasoconstriction
All major burns are going to have change in pulmonary physio even with no direct inhalational injury

What is carbon monoxide poisoning?
- Suspect with inhalational injuries; detected by measurement of arterial COHgb levels
- the severity of symptoms correlates with COHgb level
-
>30% requires high FIo2 to reduce half-life
- 4hours on RA down to 60-90 minutes with 100% Fio2
- Hyperbaric O2 considered if >25% COHgb levels
- need to go ahead and intubate patient
- 200 times greater affinity for Hgb than oxygen
-
>30% requires high FIo2 to reduce half-life
- Oxygen-Hgb dissociation curve of the remaining oxyhemoglobin shifts to the left, reducing oxygen release
- Affinity of CO for myoglobin is even greater than for hemoglobin
- binding cardiac myoglobin leads to myocardial depression, hypotension, and arrhythmias
- Metabolic acidosis at cellular level
- because oxygen delivery impated
- FALSELY ELEVATED pulse ox reading

Symptoms associated w/ specific COHgb levels?
- Symptoms noted at >20%

Anesthetic considerations for patients with burn injuries?
- Fluids
- crystalloid mainstay for early phase
- colloid considered after 24 hours
- Succinylcholine
- succ okay <24 hours
- avoid if >24 hours and up to 18 months after burn injury
- Nondepolarizing muscle relaxants
- increase dose frequency and requirements (2-5 fold)during hyperdynamic phase
- no change in reversal requirements
- Consider rocuronium > 24 hours after burn injury for RSI
- IV anesthetics
- decrease dose early phase
- increase dose hyperdynamic phase
- use multimodal therapy
- Inhalation agents
- Decrease MAC early phase
- Increase MAC hyperdynamic phase
- may be beneficial for inhalation injury (bronchodilator)
- Beta blocker
- attenuate hyperdynamic phase
- Insulin
- attenuate hyperdynamic phase burn injury

Approach to burn managmeent?
- Biphasic response to injury
- Burn shock developed 6-8 hours after injury
- hypermetabolic phase develops in several days to weeks after
- Burn treatment occurs in 3 phases
- resuscitative
- debridement and grafting)
- reconstructive

Initial airway assessment in burn patients?
- consider inhalational injury likelihood
- facial burn
- hoarseness
- evidence smoke exposure
- insepct neck and oral cavity
- gold standard airway assessment: fiberoptic bronch
- CXR is usually normal in early phase
- Early intubation when upper airway injury suspected- do not wait for decompensation

Fluid resuscitation formula in burns?
targets for fluid resus?
- All based on pt weight and % TBSA burned
- parkland formula most widely used foruma in world
- recommended fluid is LR
- 4mL/kg per percentage of TBSA in 1st 24 hours
- 1/2 of calculated volume in first 8 hours
- remained of fluid over next 16 hours
- may need dextrose containing fluid for children in early phase d/t depletion of glycogen stores
-
target fluid resus
- normal BP
- UOP 1-2mL /kg/hr
- blood lactate
- base deficit
- gastric intramucosal pH >7.32
- normal CVP/CI/O2 delivery index

Ways to secure tube in burn patient?
- ties
- suture to teeth
- tie circumferential behind patient’s head
- loop NG tube through nostril and hard palate
- suture mandible, septum., nares
- probably have surgery sew in the tube if difficult airway

