Brain Injury and Raised ICP Flashcards
What % of all cancer deaths are attributable to brain tumours?
2%
What is the typical age of onset for brain tumours?
Peak in infancy and childhood
Peak in 7th decade of life
How are brain tumours classified?
WHO classification of CNS tumours
Based on presumed cell of origin from the tumour morphology (e.g. astrocytoma, oligodendrogliom, meningioma)
What does more recent evidence about brain tumour pathogenesis suggest about its origin?
Recent evidence suggests origin from pluripotent SCs
List 5 common brain tumours, from most to least common
Neuroepithelial tumours (gliomas; 52%, majority are astrocytomas)
Metastatic tumours
Meningioma
Pituitary adenoma
Acoustic neuroma
List 4 types of neuroepithelial tumours
Astrocytoma
Ependymoma
Oligodendroglioma
Medulloblastoma
Describe the aetiology of brain tumour development; what factors may predispose and what factors are not important?
Few clearly defined environmental RFs: ionising radiation increases risk of meningioma and glioma, no role proven for electromagnetic radiation (mobile phones) or other environmental factors
FHx is rare
Some inherited/genetic conditions are predisposing: neurofibromatosis 1 and 2 predispose to multiple tumour types, Li Fraumeni syndrome (p53 loss) predisposes to glioma
Mr Xuereb, 65, was taken by his family to the GP
They are concerned that has been acting strangely; he has been complaining of a headache and has been bumping into furniture and doors at home, and had a minor car accident the day before presentation
PHx: previously well, mild treated HTN, no Sx, no cancers, smoker
Symptoms have been progressively worsening over a few weeks: headache is worse in the morning and makes him nauseated, feels better later in the morning, but if he coughs or strains the headache is exacerbated, and he has noticed some clumsiness of his R hand and a tendency to run into objects on his R side
O/E: bruising on R side of face, GCS 14 (confused to day of week and date), right homonymous hemianopia to confrontation, mild papilloedema, mild R pronator drift and hyper-reflexia
Describe the clinical presentation
DDx?
Raised ICP with focal neurological deficits, suggesting an intracranial mass enlarging over a few weeks
DDx: primary brain tumour, metastatic brain tumour, brain abscess, chronic subdural haematoma
Other causes of focal deficit (e.g. stroke) are unlikely due to time course and headache
Other causes of headache (e.g. migraine) are unlikely due to time course, associated deficits and headache characteristics
Mr Xuereb, 65, presents with features on Hx and Ex suggestive of an intracranial mass enlarging over a few weeks
Ix? What are the expected findings in a primary brain tumour?
Baseline bloods: normal
CXR (given smoking Hx and risk of secondary malignancy): normal
CTB: mass (in this case the location of the mass was deep L temporal and occipital lobes)
If CTB shows mass, grounds for immediate referral to neurosurgery and performance of an MRI
What does Mr Xuereb’s
Mr Xuereb, 65, presents with features on Hx and Ex suggestive of a progressively enlarging intracranial mass
What does his T1-weighted contrast MRI show?

Heterogeneous deep temporal mass with patchy contrast enhancement and areas of necrosis
Optic radiation and internal capsule are compressed or invaded by the tumour
Features are of a glioblastoma multiforme (thick, irregular-enhancing margins and a central necrotic core, which may also have a haemorrhagic component; surrounded by vasogenic-type oedema, which in fact usually contains infiltration by neoplastic cells)

What % of gliomas are malignant astrocytomas?
50%
What are 2 types of malignant astrocytoma and how are they graded according to the WHO classification?
Glioblastoma multiforme (WHO grade 4)
Anaplastic astrocytoma (WHO grade 3)
When do malignant astrocytomas usually arise?
6th-8th decade of life
What is the prognosis for a malignant astrocytoma?
“Dismal”
Median survival 7-14 months for glioblastoma multiforme
Median survival 2-5 months for anaplastic astrocytoma
List 6 defining histopathological features of malignant astrocytoma

What is the typical clinical presentation of an intracranial mass?
Symptoms of raised ICP (what are these?)
Seizures (seen in 40-80% of cases)
Focal neurological deficit (symptoms dependent on location of mass)
What is the duration of symptoms from an intracranial mass dependent on?
Rate of growth of mass (which is in turn dependent on grade of tumour; may anywhere between weeks and years to present)
What are the possible mechanisms of raised ICP with an intracranial mass?
Tumour mass
Surrounding oedema
Hydrocephalus (if CSF pathways are blocked)
Sx of raised ICP
Headache
N + V
Drowsiness (important sign of critically raised ICP and implies impending deterioration; alert patient with severely raised ICP may deteriorate very quickly with even a small further rise)
What are the characteristics of headache in raised ICP due to brain tumour?
Gradually progressive
Worse on waking and improves during the day
N+V as ICP rises (vomiting may temporarily relieve headache)
May be associated with drowsiness (this is an important sign of critically raised ICP and implies impending deterioration)
Describe the Monro-Kellie doctrine
Cranial cavity is a rigid boxed and increase in contents will cause a rise in pressure
There is some capacity for compensation but when a critical point is reached (circled), even small increases in volume result in large increases in ICP
The vertical section of the curve can be shifted to th left with more rapid increases in volume (e.g. expanding haematoma vs slowly growing tumour)
What focal neurological deficits may be seen in primary brain tumour and what region of the brain is affected in each?
Mood disturbance, personality change, “psychiatric” symptoms: frontal lobes (especially seen in “butterfly glioma”, affecting both frontal lobes)
Limb weakness: motor cortex in posterior frontal lobe or deep pyramidal pathways (internal capsule, brainstem)
Visual field defect: occipital, temporal or parietal lobes (anywhere along the visual pathway)
Dysphasia: dominant frontal or temporal lobe (usually L)
NB Brainstem lesions can cause multiple deficits including weakness, sensory loss, diplopia and cranial nerve deficits
Principles of Mx of malignant astrocytoma
Commence steroids (dexamethasone) to reduce cerebral oedema and ICP
Resection of as much of tumour as is safely possible (if not possible then biopsy only)
Adjuvant therapy: radiotherapy, chemotherapy (given in various combinations depending on tumour grade)
What is the aim of surgical resection for malignant astrocytoma?
Tissue Dx (essential!)
Resection of all of visible tumour (if possible; will still leave microscopic tumour but will reduce mass effect and symptoms, provide tissue for banking and research)

Why might surgical resection of a malignant astrocytoma not be possible?
Tumour extent (large, diffuse)
Tumour location (eloquent brain; areas of cortex that—if removed—will result in loss of sensory processing or linguistic ability, minor paralysis, or paralysis)
Patient age or fitness for surgery
Give an example of a radiotherapy regime used postoperatively for malignant astrocytoma
45-60 Gy (gray; unit of ionising radiation) in 20-30 fractions, delivered to tumour bed + 2cm margin
What is the benefit of radiotherapy in the Mx of malignant astrocytoma?
Level 1 evidence it prolongs survival
What chemotherapy drug is commonly used for treatment of malignant astrocytoma and what are the benefits of this drug?
Temozolomide
Oral, lower SE profile than previously used chemotherapy
Often given concomitant with radiotherapy
What clinical features may confer an even poorer prognosis in malignant astrocytoma?
Older age at Dx (esp >65 years)
Poor neurological condition at Dx
Higher grade
Incomplete surgical removal
Mr Nguyen, 39, was taken by his family to the GP; they are concerned he has been acting strangely, with episodes of staring into space and also of “panic attacks”
He had been found in bed that morning having wet the bed and was slightly confused, with blood around his mouth
PHx: previously well but long Hx of “panic attacks” where he stares into space and makes chewing movements before being overwhelmed by a feeling of dread that makes him want to run from the room (he then becomes extremely tired)
No headache, N+V, other neurological symptoms
O/E: normal neurological examination
What is this clinical presentation and what are the next steps for the GP?
Complex partial seizures previously, with a generalised seizure this morning
Arranges urgent review by neurologist in ED, where he was commenced on anti-convulsants and an MRI scan was arranged
Mr Nguyen, 39, was taken by his family to the GP; they are concerned he has been acting strangely, with episodes of staring into space and also of “panic attacks”
He had been found in bed that morning having wet the bed and was slightly confused, with blood around his mouth
A FLAIR and T1-weighted MRI with contrast was organised. What are the findings and what are these features suggestive of?
Homogeneous mass best seen on FLAIR/T2-weighted MRI with no contrast enhancement and minimal mass effect
Findings consistent with a low grade glioma

Histopathological findings in low grade glioma
As for malignant astrocytoma but less abnormality in terms of the hypercellularity, and cellular and nuclear atypia/pleiomorphism
Very few mitoses
No necrosis
Invades diffusely through the normal brain
May have calcifications
What kinds of tumours are classified as low grade gliomas and what is their grade under the WHO system of classification?
Includes oligodendrogliomas, astrocytomas and mixed forms
WHO grade 1 (usually children) and 2 (adults)
What is the typical age group affected by low grade glioma? What is the typical presentation?
Patients are young (25-45)
Presentation: neurologically intact, often only with seizures
Prognosis of low grade glioma
Survival is prolonged (years to decades) but eventual growth of low grade tumour or progression to a higher grade will occur
Describe the principles of Mx of low grade glioma
As patients are young and neurologically intact with prolonged survival, SEs of treatment are important and should be avoided:
Removal of as much tumour as safely possible (or often only a biopsy to avoid deficit)
Tissue Dx essential
Defer radiotherapy and chemotherapy until tumour progression
Mrs Zhu, 61, was treated for smoking-related lung cancer 1 year ago; she is reasonably well, but continues to smoke, and for the last week has noticed difficulty saying some words
O/E: expressive dysphasia. mild R sided weakness
What are the feaures of an expressive dysphasia? Ix?
Expressive dysphasia: difficulty naming objects but no difficult following commands
Ix: CT and, if abnormal, MRI
Mrs Zhu, 61, was treated for smoking-related lung cancer 1 year ago; she is reasonably well, but continues to smoke, and for the last week has noticed difficulty saying some words
CTB and MRI (T1-weighted and FLAIR) were performed
What are the findings?


What % of brain tumours in clinical series are metastatic?
15% (but actually more common; frequently present at autopsy in cancer patients, frequently not treated)
What proportion of metastatic brain tumours are solitary vs multiple?
1/3 solitary
2/3 multiple
What pathological process is often responsible for the symptoms seen in metastatic brain tumour? Is it solely due to the presence of a space-occupying lesion?
Often the intense cerebral oedema is the cause of more symptoms than the tumour mass
List 5 primary tumours which commonly metastasise to brain
Lung
Breast
Melanoma
Kidney
GI carcinoma
NB In 15% of cases, the primary is unknown
What region of the brain is commonly affected by metastatic tumour?
Cerebellum (may cause obstructive hydrocephalus)
What is the presentation typically seen with a metastatic brain tumour?
Similar to any mass: raised ICP, focal deficit, seizures
Mx of brain metastases
Commence steroids (dexamethasone) to reduce cerebral oedema and ICP
Surgery to remove the metastasis if solitary, and if primary disease is stable and patient has reasonable a life expectancy (if primary cancer is unknown, brain met should be removed to confirm the Dx)
Occasionally one of multiple mets will be removed for palliation (if it is causing disabling symptoms, e.g. hemiparesis, that can be improved by removal, even if the patient may only live a few months)
Whole brain radiotherapy (45 Gy) for multiple metastases or after removal of a single metastasis (controversial)
Stereotactic radiotherapy (single high dose focussed radiation for 1-3 metastases)
Chemotherapy and targeted agents generally have poor penetration in the brain
What is myokymia?
Involuntary, spontaneous, localised quivering of a few muscles, or bundles within a muscle, but which is insufficient to move a joint
Mrs Khoury, 60, presents to her GP complaining of twitching of her R eyelid; sounds like typical benign myokymia and neurological examination is normal
She has no headaches; however, Mrs Khoury is very concerned she has a brain tumour as her brother died of a brain tumour
She insists on an MRI
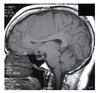
What are the findings?

T1-weighted sagittal MRI without contrast shows a huge mass that appears extra-axial (outside the brain)
T1-weighted sagittal MRI with contrast (not shown) demonstrates huge mass that appears attached to the falx and has well demarcated margins
What is the most common benign brain tumour?
Meningioma
In what population groups is meningioma most common?
Middle age
Women > men
What is meningioma? Where do they characteristically occur?
Benign brain tumour arising from arachnoid cells in the meninges and which occurs in characteristic locations on the dura (most commonly falx, convexity and sphenoid wing; each location has a characteristic clinical syndrome)
Often associated with intense oedema
Describe the histopathology of meningioma
“Whorls” are a common feature

What is the significance of subtyping of meningiomas?
Generally no prognostic significance; a few subtypes portend a poorer prognosis
Is malignancy common in meningioma?
No, malignancy is infrequent
How do meningiomas present?
As for any intracranial mass: raised ICP, seizures, focal neurological deficit (dependent on location)
Describe the natural Hx of meningioma
Slow-growing, therefore may reach a very large size
Symptoms may be present for years
May be asymptomatic and discovered incidentally
Principles of Mx of meningioma
Total surgical excision and obliteration of the dural attachment is the most effective treatment (extent of resection is related to risk of recurrence)
If complete excision not possible, subtotal excision and diathermy of dural attachment
Radiosurgery or radiotherapy for small, residual, recurrent or malignant tumours
