Define Metaplasia distinguish between different types and give an example
A reversible change in which one adult cell type (usually epithelial) is replaced by another adult cell type
- This is usually adaptive change
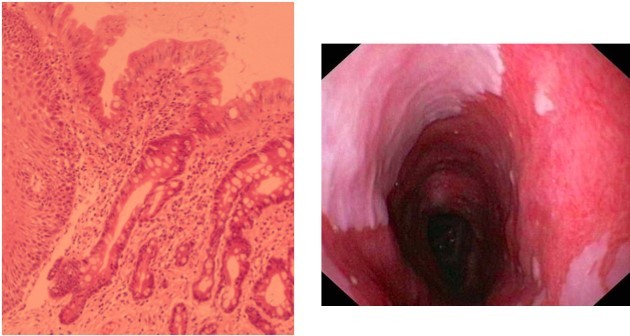
- Example: Barrett’s Oesophagus - gastro-oesophageal reflux causes the oesophageal epithelium to change from squamous to columnar (NOTE: this is pathological metaplasia)
- You can get physiological metaplasia e.g. in pregnancy the cervix opens up and the columnar epithelium of the endocervical canal is exposed to the acidic uterine fluids making it become squamous
- When the cervix closes up again, the cell type changes back to normal (hence why metaplasia is a REVERSIBLE change)
Define Dysplasia, state its main features, results and which tissues are more affected
An abnormal pattern of growth in which some of the cellular and architectural features of malignancy are present (different from metaplasia but occur at the same site, ex. Oesophagus)
- Cancer is a multi-step process so there must be some steps in between normal and cancer
- The cells in dysplasia are on the road to cancer but haven’t reached it yet (cancer is a multistep process)
- Dysplasia is a pre-invasive stage with an intact basement membrane
- Dysplasia can be used to screen for cancer, to pick up high risk individuals before they get full-blown cancer
What happens in Dysplasia?
- There is a loss of architectural orientation
- There is a loss of uniformity of individual cells
- Nuclei are hyperchromatic and enlarged
- Mitotic figures are abundant, abnormal and in places where they aren’t usually found
- Everything becomes more variable
- Increased nucleo-cytoplasmic ratio
Dysplasia is common in:
- Cervix - HPV infection (HPV is associated with the greatest risk of developing cancer)
- Bronchus - smoking
- Colon - ulcerative collitis
- Larynx - smoking
- Stomach - pernicious anaemia
- Oesophagus - acid reflux (metaplasia first and then dysplasia)
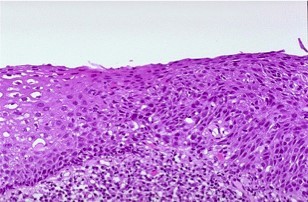
- This is a cervical biopsy
- On the left you can see that the cells are very compact at the bottom then become more and more spaced out towards the lumen - normal cellular maturation
- On the right hand side of this image, the cells are NOT undergoing normal maturation
- There are compact cells with dark, dense nuclei on the surface - these cells are normally seen further down
State the difference between Low Grade and High Grade Dysplasia
- Low Grade - low risk of progression to cancer, more likely to be easily treated
- High Grade - high risk of progression to cancer (nucleus cytoplasmic layer is higher–> hyperchromia)
- Difference between low grade and high grade: both show changes of dysplasia, but the changes are more severe in high grade dysplasia
- The nuclei are bigger, and the nucleo-cytoplasmic ratio is higher in high grade dysplasia
State the most common characteristics of a Benign Tumours, how can they prove dangerous?
Benign
- DO NOT INVADE and DO NOT METASTASISE (they don’t invade blood vessels)
- Slowly growing
- Normal mitotic figures
- Encapsulated - they have a compressed capsule around them (easily removed)
- Exception: fibroids (leiomyoma) in the uterus does NOT have a capsule
- ‘Well differentiated’ = they look like the tissues that they come from
- Above is a fibroadenoma of the breast tissue - it is sharply demarcated and is well differentiated
- If the tumor is not attached to skin or any structure then it is not bad
- Benign tumours do NOT tend to be fatal unless they:
- Are in a dangerous location
- E.g. meninges, pituitary (brain), block the flow of CFS from the lateral and third ventricle you will give hydrocephalous
- Secrete something dangerous
- E.g. insulinoma
- Gets infected
- E.g. bladder (whenever you block anything that drains fluid, you will create the conditions for infection), it can bleed (it can oress into an artery, they can rapture, torts )
- Bleeds
- E.g. stomach
- Ruptures
- E.g. liver adenoma (can cause massive haemoperitoneum)
- Torts (twisted)
- E.g. ovarian cyst
- Are in a dangerous location

Define Neoplasia, Tumour and Malignancy
- Neoplasia = any new growth, benign or malignant
- Tumour = swelling (e.g. nasal polyps are also considered tumours)
- Malignancy = an abnormal, autonomous proliferation of cells, unresponsive to normal growth control mechanisms
- Example: in the oestrogenic phase of the menstrual cycle, the endometrial epithelium proliferates. When the oestrogen levels drop, the proliferation should stop. But in cancer, the controls have become autonomous and can’t easily be switched off.
What are the main characteristics of Malignant Tumours ?
- INVADE SURROUNDING TISSUES
- SPREAD TO DISTANT SITES, metastasis
- No capsule
- Well to poorly differentiated
- Rapidly growing
- Abnormal mitoses
Define Metastasis, what is the most important determinant?
Metastasis - a discontinuous growing colony of tumour cells, at some distance from the primary cancer (they break off from the primary tumour and then travels to another location)
- The prognosis of a cancer is very much dependent on whether it has spread
- The sites of metastasis depends on the lymphatic and vascular drainage of the primary site
- Example: the pancreas is drained by the splenic vein, which then goes via the hepatic portal vein to the liver so pancreatic carcinomas tend to present with liver metastases
- Lymph node involvement has a worse prognosis
- Example: Colon cancer (uses Dukes staging system)
- Dukes A - 90% survival (confined to bowel wall)
- Dukes C - 30% survival (lymph node involvement)
- Breast–>maxiallry lymph nodes
Which is the basic Nomenclature of Tumours?
- Benign epithelial tumours
- Carcinoma
- Benign soft tissue tumours
- Sarcoma
- Leukaemia & Lymphoma
- Teratoma
- Hamartoma
What is the distinction of Benign Epithelial Tumours?
- Of SURFACE epithelium = PAPILLOMA
- E.g. skin, bladder
- Of GLANDULAR epithelium = ADENOMA
- E.g. stomach, thyroid, colon, kidney, pituitary, pancreas
Define Carcinoma, how can we divided into types?
- A malignant tumour derived from epithelium
- Adenomas could become adenocarcinomas
- Types of carcinoma: (based on the epithelium it has derived)
- Squamous cell carcinoma
- Adenocarcinoma
- Transitional cell carcinoma (transitional epithelium is found in the bladder)
- Basal cell carcinoma
- So we classify tumours based on the tissues that they come from
What are some examples of Benign Soft Tissue Tumours?
- Bone - osteoma
- Fat - lipoma
- Smooth Muscle - leiomyoma
Define Sarcoma, state some possible sarcomas
- A malignant tumour derived from connective tissue (mesenchymal) cells
- The prefix is the site of the tumour e.g. osteosarcoma (bone)
- Types of sarcoma:
- Fat = liposarcoma
- Bone = osteosarcoma
- Cartilage = chondrosarcoma
- Striated Muscle = rhabdomyosarcoma
- Smooth Muscle = leiomyosarcoma
- Nerve Sheath = Malignant Peripheral Nerve Sheath Tumour
Distinguish between Leukaemia and Lymphoma
- These are both tumours of white blood cells
- Leukaemia - malignant tumour of BONE MARROW derived cells which circulate in the blood
- Lymphoma - malignant tumour of LYMPHOCYTES (usually) IN LYMPH NODES
- NOTE: lymphocytes are produced by the bone marrow and they are found in lymph nodes so in some cases you can get a mix of both lymphoma and leukaemia
Define Teratoma, what is the differentiation pattern? (state a gender difference)
- A tumour derived from GERM CELLS, which has the potential to develop into tumours of ALL THREE germ cell layers (it is always foinf ectopically)
- Any tissue in the body can be found
- Three Layers: Ectoderm, Mesoderm + Endoderm
- All the slides on the left are from ONE tumour
- There are loads of different cell types in one teratoma
- IMPORTANT NOTE:
- Gonadal teratomas in MALES are almost ALL MALIGNANT
- Gonadal teratomas in females are mostly benign
Define Hamartoma, when is it more common?
- Definition: localised overgrowth of cells and tissues NATIVE TO THE ORGAN (it is disorganised but it is normal)
- In other words: the tissues that are present are appropriate for that particular part of the body but the way that they are architecturally arranged is inappropriate
- Architecturally abnormal
- The cells are mature but architecturally abnormal
- This is common in children, and should stop growing when they stop growing
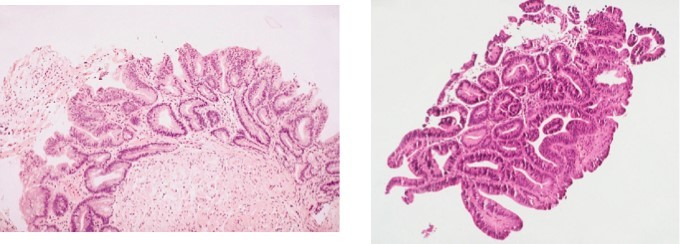
- Example above:
- This is a section of liver showing the bile ducts
- A normal portal tract only contains ONE bile duct
- Here there are loads of bile ducts
- Normal bile ducts are round but these ones are a little misshapen
- Though there are no issues cytologically
- These bile ducts are abnormally arranged
What is the difference berween benign and malignat
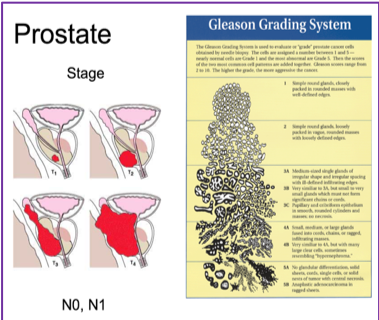
Grading Vs Staging
- Grade – describes degree of differentiation.
- Stage – describes how far it has spread.
- Higher grade tends to mean higher stage.
- Stage is MORE important than grades (for prognosis determining).
- TNM can be applied to tumours at all sites.
-
Basic Terminology17
-
Cell Cycle25
-
Signalling Mechanisms in Growth and division18
-
Signalling Mechanisms in growth and divisions: part 221
-
Oncogenes and tumour Suppressants19
-
Apoptosis30
-
Angiogenesis19
-
DNA Damage and repair21
-
Biological Basis of Cancer Therapy22
-
Invasion and regulation of motility17
-
External Factors28
-
Cancer Epidemiology10
-
Breast Cancer15
-
Colorectal Cancer6
-
Skin Cancer9
-
Leukaemia4
-
Prostate Cancer4
-
Questions for Cancer examples4
