Asthma?
Chronic inflammatory airway disease characterised by variable reversible airway obstruction, airway hyper-responsiveness and bronchial inflammation.
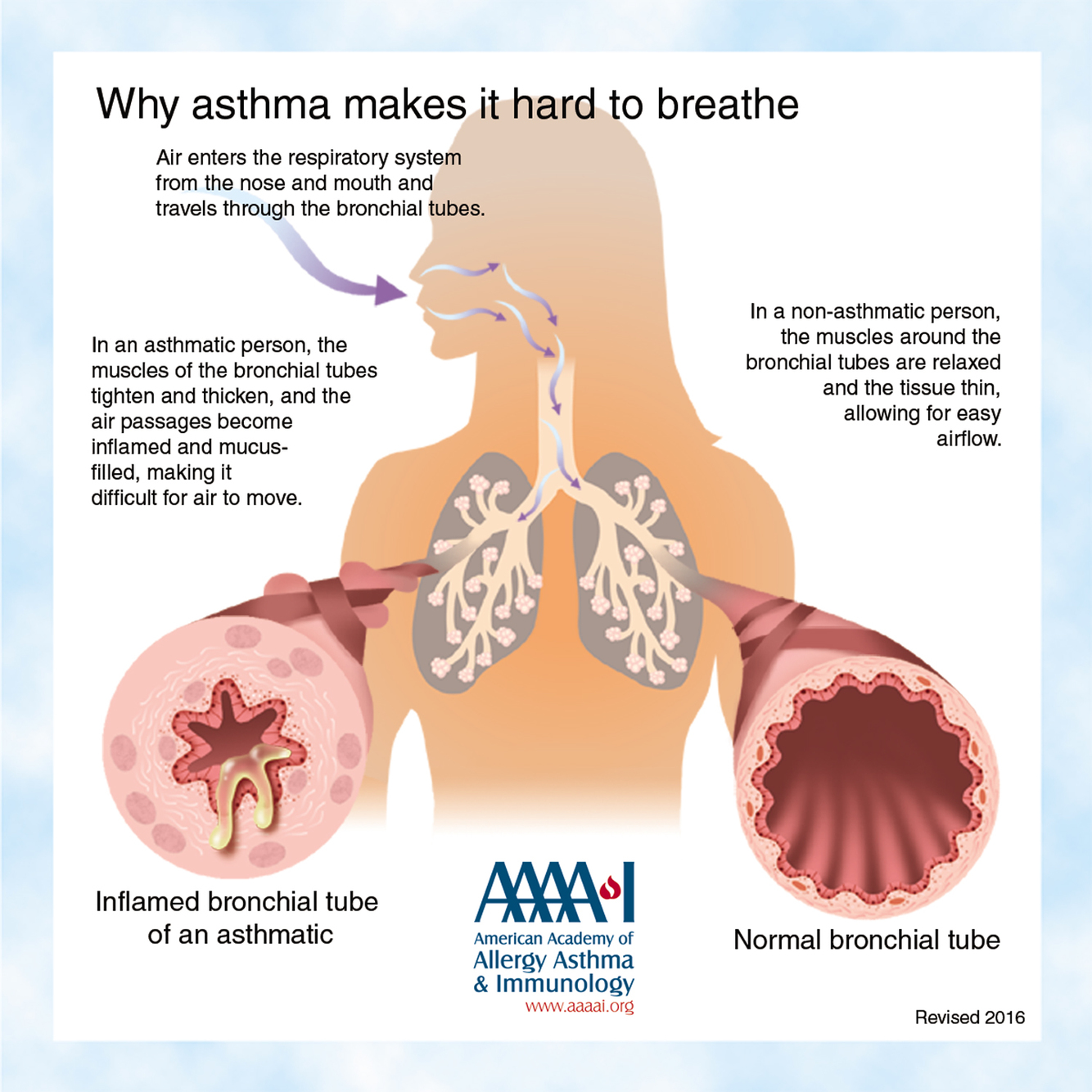
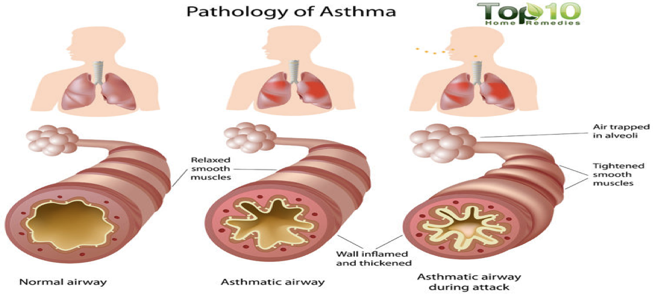
Asthma pathology?
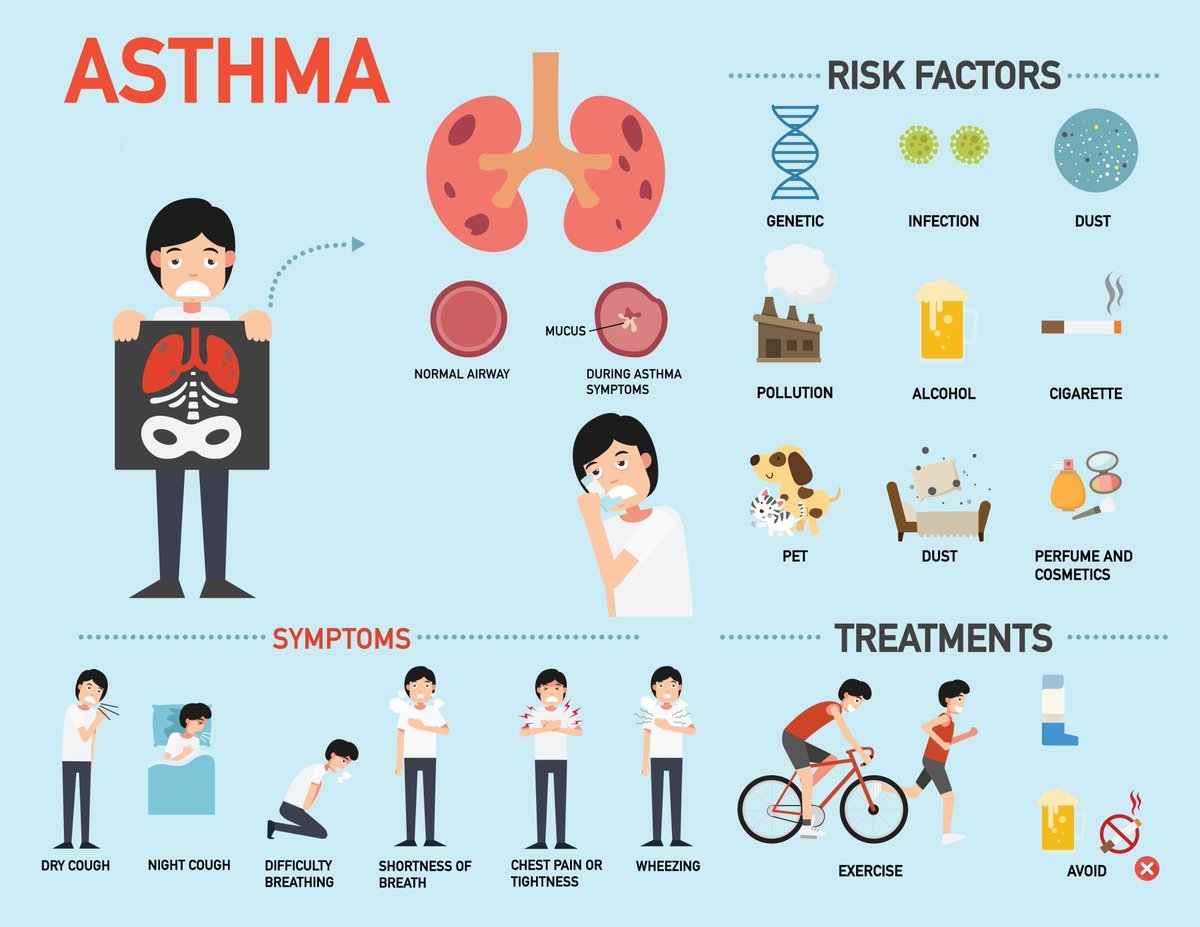
Asthma risk factors (9)?
family history, atopy, house dust mites, pollen, pets, cigarettes, viral resp tract infections, occupational allergens.
Asthma epidemiology?
10% of hildren, 5% of adults
Asthma precipitating factors (5)?
Cold,
viral infection,
drugs (e.g. beta-blockers, NSAIDs),
exercise,
emotions
Asthma symptoms?
episodic history, wheeze, breathlessness, cough
Asthma signs (5)?
tachypnoea, use of accessory muscles, prolonged expiratory phase, polyphonic wheeze, hyperinflated chest.
Asthma signs of a severe attack (4)?
PEFR < 50%
predicted Pulse > 110/min
RR > 25/min
Inability to complete sentences
Asthma signs of a life threatening attack (7)?
PEFR < 33% predicted
silent chest
cyanosis
bradycardia
hypotension
confusion
coma
Asthma investigations?
Peak flow, pulse oximetry, ABG, CXR, FBC, CRP, U&Es, Blood and sputum cultures.
Asthma management acute?
ABCDE, resusitate,
high-flow O2, salbutamol nebulizer, ipratropium bromide, steroid therapy (hydrocortisone followed by prednisalone)
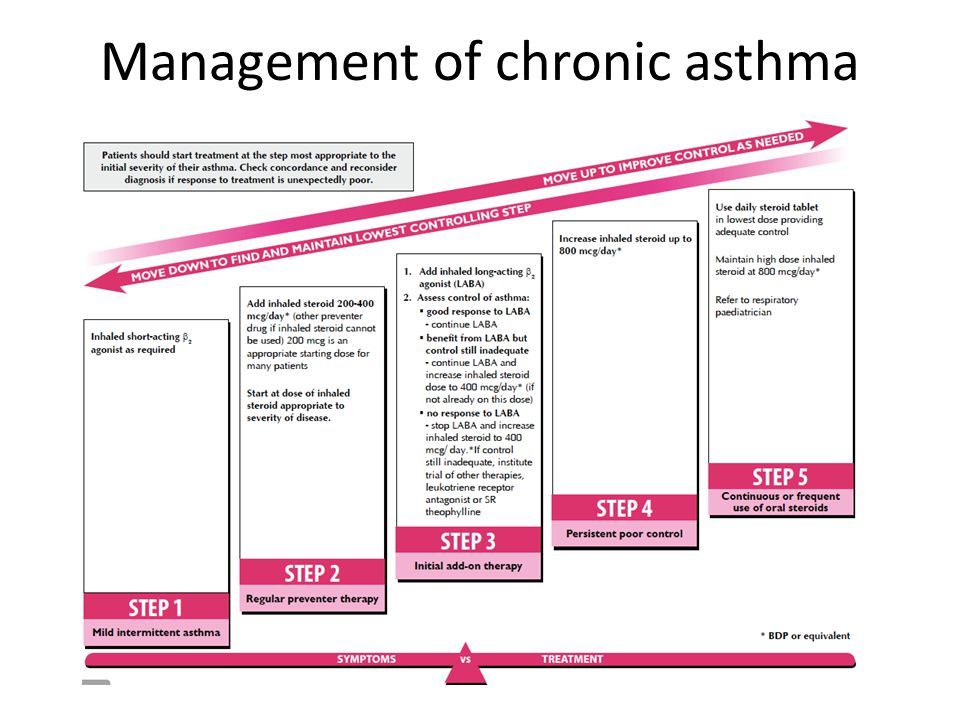
Asthma management chronic step 1?
Inhaled short-acting beta-2 agonist used as needed
If needed > 1/day then move onto step 2
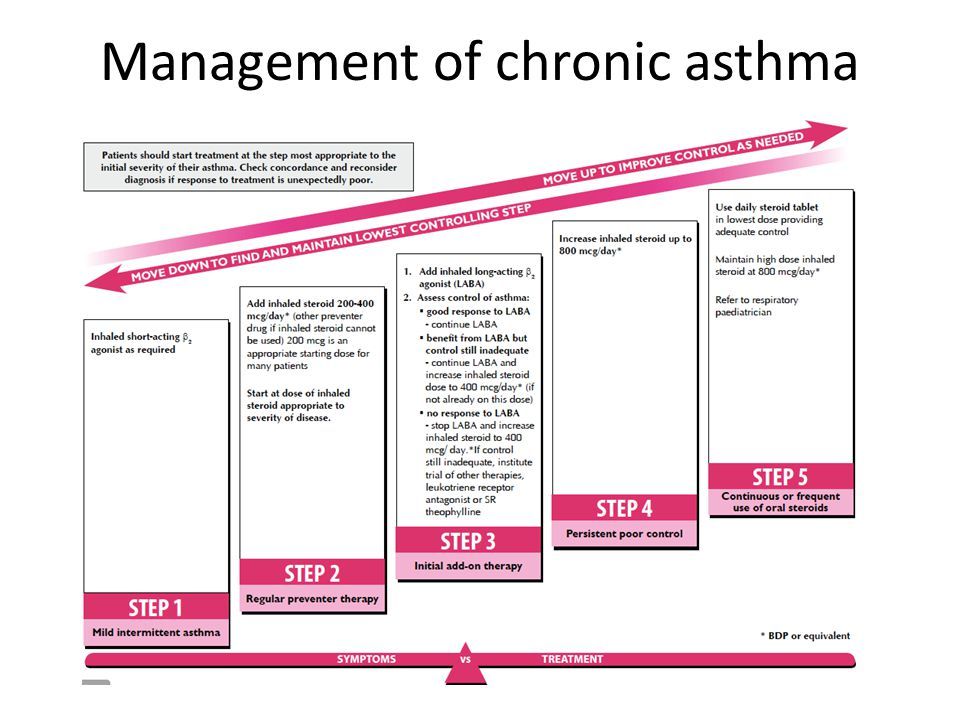
Asthma management chronic step 2?
Step 1 + regular inhaled low-dose steroids (400 mcg/day)
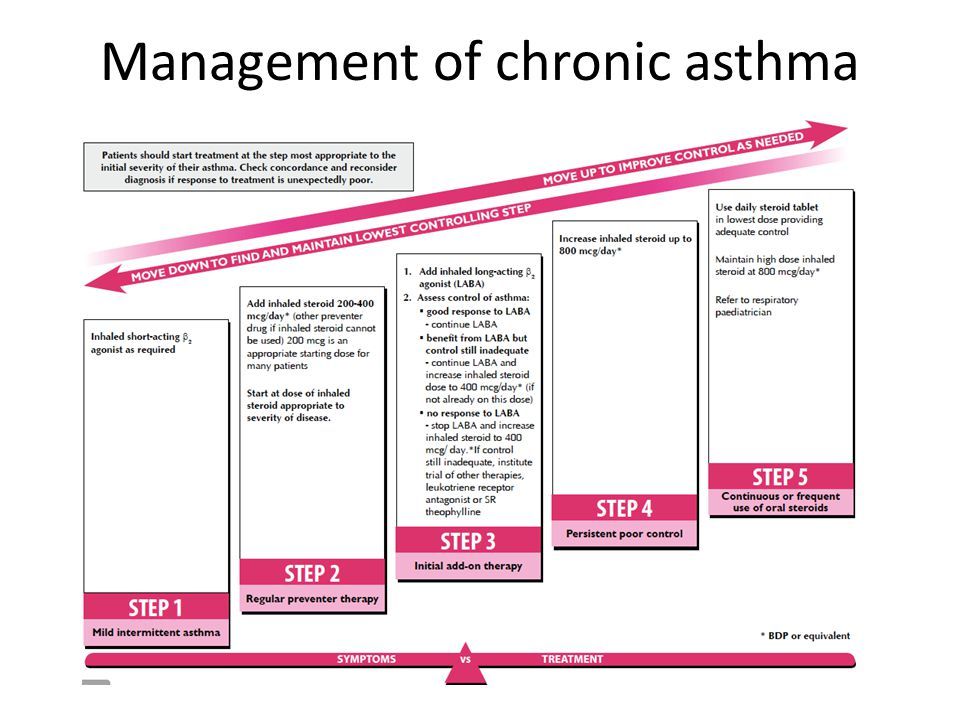
Asthma management chronic step 3?
Step 2 + inhaled long-acting beta-2 agonist (LABA)
If inadequate control with LABA, increase steroid dose (800 mcg/day)
If no response to LABA, stop LABA and increase steroid dose (800 mcg/day)
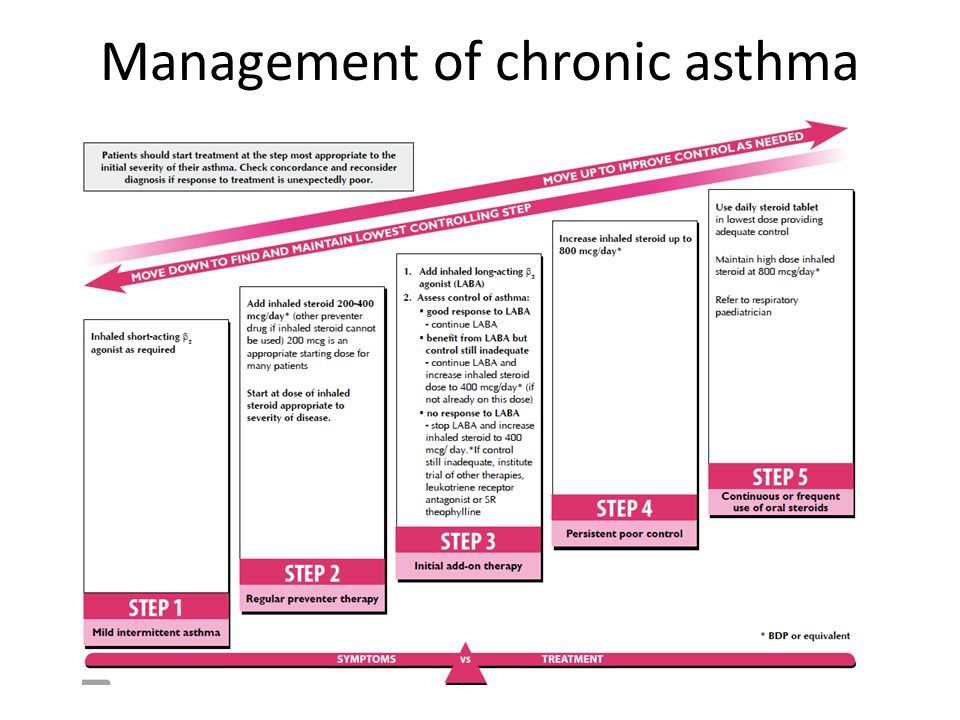
Asthma management chronic step 4?
Increase inhaled steroid dose (2000 mcg/day)
Add 4th drug (e.g. leukotriene antagonist, slow-release theophylline or beta-2
agonist tablet)
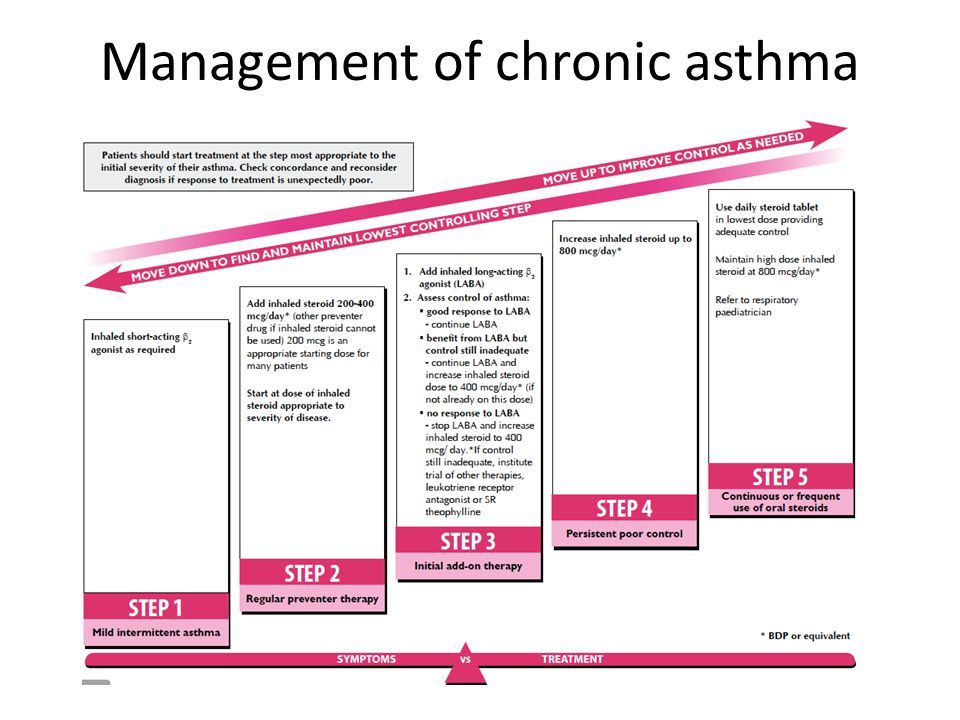
Asthma management chronic step 5?
Add regular oral steroids Maintain high-dose oral steroids Refer to specialist care
Asthma complications (6)?
Growth retardation, chest wall deformity, recurrant infections, pneumothorax, respiratory failure, death.
