Antimicrobial Drugs Flashcards
How Antibiotic Resistance Happens
- Antibiotics were discovered and first really used in the 20s
- Every decade there is resistance that has started to appear
- We have companies that want drugs to be used a lot (this is their product!), but we HAVE to limit our use of antibiotics
- note: dont use the word germs
- there is always resistant bacteria around, but we need to keep some competition present!

Examples of how Antibiotic Resistance Spreads
- eating meat with antibiotic resistant bacteria
- hard to know the exact role of pets in all this but they are part of it and can get resistant bacteria from owner!

Goal of Antibacterial Therapy
- not every infection needs antibiotics
- when we use them appropriately, they are to HELP the host rid of the infectious organism
- bacterial cells are different to the mammalian cell
- where as: it is hard to treat cancer cells as they are similar to the host and the drug is therefore somewhat toxic

Antibiotic therapy is most effective when…

Natural Defence Mechs of Patient
- If M.E. is damaged, they are very prone to building respiratory tract infections
- UTIs can occur for people with renal issues

Bacterial Resistance and Antibacterial Agents
- bacterial resistance existed well before antibiotics were invented!

Bacterial resistance
- Bacteria have been killing eachother with “antibiotics” for ages to kill other bacteria!
- A good amount of the antibiotics come from fungi (e.g. penicillin)

Resistance and Antibiotic selection
- resistance does not just emerge at the site of infection but the normal flora in the gut and the skin

The Gut Microbe- What does it do and why do we care?
- what happens if the gut/skin microbiome are altered by antibiotics
- both (esp. gut) is very important for the immune system and body function
- basically signals to the immune system what is ok to have in body and what isnt

Immune system and cohabiting microbiota

- Dysbiosis= when microbiome of the gut/skin become disordered and arent at the amount they should be
- loss of control by the gut and immune system
- often a mix of all these
Bigger Picture: increased prevelance in people
- Increasing in prevelance despite the fact of knowing more and more about these diseases

People with Immune Mediated Diseases
- Diseases we didnt think were immune mediated did start as immune mediated in many cases
- start with a different microbiota
- meaning antibiotics can have an effect in these situations

Antibiotics and the microbiome

Whether an antibiotic is used appropriately or not…
- we will cause resistance either way
- is the benefit going to outweigh the fact that you are going to change the microbiota
- use of antibiotics in the early stages of life seem to have the largest impact on the immune system and functionality of animal/human

Responsibility of Veterinarian
- antibiotics dont cause many side effects as they are aimed at bacterial cells, not mammalian cells (different to anti-cancer drugs, NSAIDS)
- Vets have used lightly before as there arent really any side effects to mammalian cells
- disease prevention: worming suggestions, diet, etc.
- conservatively: treat with the right dose at the right time only when needed!

Issues for food animals

Horses
- MUST be signed out or it has to be treated as a food animal

Food animals and Drug Residues
- Drugs have a calculated withdrawal time: time where drug administration has stopped and when the animal is able to be slaughtered
- REALLY try to avoid the use of antibiotics in food animals, or be very strict about it!
- even the smallest bit of antibiotics (ex: penicillin) can cause an allergic reaction in people who consume products

Food Animals and Withdrawal times
- times are stated for all registered drugs
- the criteria MUST be followed for that withdrawal period to work
- If you are giving antibiotics for an animal destined for slaughter and production, you MUST look at data sheet

If not licensed: The Cascade

- There are a lot of times where the drugs may not be licensed for a certain condition or species
- you as a vet need to make a risk based clinical judgement: happens all the time!
- need to get owner consent
- for food animals: need to have an MRL and need to be able to specify the MINIMUM withdrawal time
- also keep records of treatment

If not licensed in food animals?
- these withdrawal periods are set by LAW
- use in food animals still applies the needed use of antibiotics in general, but the added layer of withdrawal times

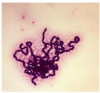
Gram Staining

Microbial Spectrum
- 4 quadrants
- gram (-) aerobe: like E.Coli
- Penicillinase producing staph is really important!

- gram + aerobic bacteria - STREP

- Gram Negative aerobic bacteria

- Staph aureus
Atypical Bacteria Species
(6)
- they don’t gram stain!
enormously important as a causes of a variety of diseases depend on which area you are practicing in

Antimicrobial classes: Inhibition of Cell Wall Synthesis
(3)
- knowing the mech of action doesnt reallyyy change how much we use them, but it is important in our clinical reasoning
- bacitracin: in ear drops

Antimicrobial Classes: Inhibition of Cell Membrane Function
(4)
- most of these are anti-fungal drugs and not antibiotics!
Classes: Inhibition of Protein Synthesis
(5)
- chloramphenicol
- macrolides
- lincosamides
- tetracyclines -commonly used
- aminoglycosides
- these do have the capacity to change mammalian protein synthesis but much lower affinity for mammalian cells!

Classes: Inhibition of Nucleic Acid Synthesis
(5)
- chunking them doesnt matter a lot of the time, but helps to put them into groups to remember them!

When to use antimicrobials?
- only when you definitely diagnose a bacterial infection that needs treatment
- would cause critical illness and would progress if we do not treat it

Key Q’s and Clues: bacterial infection
- what are you looking for in clues? - signs of bacterial infection!
- increased body temp can ALSO occur in situations of cancer, or other illnesses (not a hard fast sign)
- neutrophil increase can happen in non-bacterial inflammation, stress, cancer

Antibiotics not indicated for….
- vomiting/no diarrhea: likely do not have a bacterial disease even if they ingested most disgusting items
- urine in cats is very hostile to bacteria (echo) - often environmental/stress. OVER ten years, urine becomes more dilute and then they are more prone to bacterial infections
- huge misconception: blood in feces needs antibiotics. not necessarily a bacterial infection causing blood to be in feces
- peridontal disease: commonly given AB’s before, during, after–> mechanically clean teeth!! don’t use the AB’s- biofilms

Choosing the right antibacterial drug
- can use guidelines, but you need to understand why those drugs are appropriate
- prescribe based on what is the most likely bacteria you are going to run into in the area of issue
- culture and sensitivity? is it recurrent?

Key Questions to Ask
(8)
*

Factors Affecting the Success of Antibacterial Therapy

Where do infections come from?
- A lot of the time the bacteria comes from within and gets to a place where it shouldnt be or they are in same area but the is not enough restriction placed by the body–> become a pathogen

Infection based on location
- gram (-) aerobes and anaerobes in large bowel?
- liver: coming from up the biliary tract or systemically (which would be staph)

What groups of bacteria live in the gut?
What Bacteria live on the skin?
Examples of gram (-) bacteria that cause disease in animals
Bacterial Susceptibility
- Strep is dumb - hasnt developed much
- gram negatives can be very unpredictable on the other hand in their sensitivity patterns

MIC
- helps us determine sensitivity pattern
- lowest effective dose!
- Drug brands have to name the bacteria that show sensitivity to that drug
- also need to be aware which slow growth and which kill
- issues: really only applies in lab settings and is inconsistent

Bacteriostatic vs bactericidal?
- can really tell if bacteriacidal is better than bacteriostatic drugs: especially in terms of gram (+) infections

Bacteriostatic Drugs
- For these drugs to be clinically effective, the drug concentration needs to be above the MIC for the duration of treatment or else the bacterial population will continue to grow
- need to stress the importance of timing of these doses!

Bacteriostatic
(5)
- These are what they are broadly

Bactericidal
- don’t need ideal conditions?
- Good if we are concerned that these animals are immunocompromised or the infection is at a specific site

Bactericidal
(6)
- when all is working well, they are bactericidal
Bactericidal Killing
- How do these drugs kill the bacteria?
- can be done in a time dependent manner or dose (concentration) dependent manner

Time Dependent

- want that drug to be above the MIC throughout the dosing period
- 3 bactericidals by time dependent killing mechanisms
- cant give with a drug that slows down growth because they are only effective against a growing population of bacteria!
- Can’t give one dose as the concentration decreases too much before the end of the 24hr period - thus we want to give this dose twice in 12 hour periods! (graph)
- Don’t say give twice a day –> need to say EVERY 12 hours

Concentration Dependent
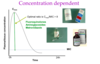
- determined by the peak concentration achieved- can combine with bacteriostatic drugs!
- don’t depend on bacteria growing
- needs to be 8-10 times more than the MIC to be effective
- doesn’t matter that it is gone before 24 hours, but main thing is that their effec tis through concentration!
- Hamsters/rabbits: tend to give it twice a day in really small animals as they have very high metabolisms and time of action is much faster

Red Antibacterial Activity

Spectrum - Red Drugs

- all the dots represent bacteria
- if they are mostly in red as you are talking about a drug, wont be affective against those bacteria species
- REMEMBER THIS MOST OF ALL
- Fluoroquinolones and aminoglycosides have no effect against obligate anaerobes
- Penicillin/aminopenicillins don’t work against pen. producing staph and metranidazole does not work in anaerobic conditions? (echo)

Green and Blue Antibacterial
- Once they have had multiple courses of antibiotics, this won’t work as the pattern of resistance has changed

Spectrum- Green Drugs

- The more that a drug is used, the more you will see red dots appear

Brown Antibacterials

Brown Drugs

- there is a mixture
- don’t memorize
- but they are not red/not green

Brown Drugs and the Empirical Choice
- don’t use if you aren’tsure what the bacterial infection is!!

Atypical Bacteria

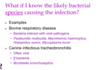
What if I know the likely bacterial species causing the infection?
- Bordatella becoming an issue because so many dogs are getting treated by AB’s
Pharmacokinetic Factors


Difficult to Access Areas

Intracellular bacteria
- need to be lipid soluble to get in the cell!!

How well do they penetrate?
- good= good enough at passing the membrane
- Great= VERY LIPID SOLUBLE
- If we are choosing to treat a brain infection, bronchiole infection, iron infection systemically –> needs to come from blues and greens!

Environmental Conditions
- What has happened at the site of infection to prevent a drug from working properly
- need to drain an abcess before giving AB
- foreign material : stone, devitalized part of bone, splinter

Foreign Material (pharmacodynamics)

- body has to fight two battles

Effects of Env’t Conditions

Post Operative Infection Risk
- health of the tissue involves the effect of the surgery itself as well
- there is a gradation of asepsis

When should I use perioperative antibiotics?

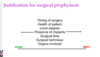
Justification for surgical prophylaxis
Post Op Risk: Surgeon and Implants
Post Operative Infection risk factors

- patients are shocked/emaciated have a higher risk

Post Op Infection risk: Anaesthesia and propofol

Post Op Infection Risk Factors: clipping, etc
- Just can’t clip as well when you they are awake
- Abnormal skin will lead to staph possibly populating and invading the area

- Indications for Surgical Prophylaxis

- In places where the aseptic technique is not as great, it is BETTER and CHEAPER to fix the aseptic technique before just giving them ABs
- dentals? - (diseases where they are more at risk to develop infection after dental) –> hypoadrenocorticism patients maybe, mitral valve disease
- patients with a low WBC
- ortho procedures usually get pre and then repeated if it goes longer than 90 min (surgery time) and after? - consequences would be disastrous
Timing of Surgical Prophylaxis
- depending on what drug is given, you ideally give it at the time of induction as there is no delay
- if it is given SQ or IM then it can take about 1-2 hours to take effect
- Has to be present in the wound at the time of contamination!

Best Drug for Surgical Prophylaxis?
- 2nd gen cephalosporin- not licensed vet med, owner will have to give consent, but it has a lot of benefits
- formulaitons may be different in different regions of the world - need to adapt
- IV induction IF possible (can take an hour and half for amoxycillin caluvulanate to reach therapeutic level)

Surgical continuation therapy
- supposed to act like a security guard checking for any intruders, but don’t continue giving afterwards
- We are treating an infection, we are preventing the infection from occurring

Major Factors influencing postop infection risk:

Where would these pathogens be coming from?
(surgical Prophylaxis)
Skin is a big one! (surgeon and animal!)
- also depends on what surgery it is
- need to think about the likely contaminating pathogens

What is the most useless drug to use for surgical prophylaxis in most SA cases?
- Amoxycillin (at least in 70% of cases- penicillinase producing)
- It is no good against staph!
- staph is one of the main concerns of surgical prophylaxis
- never use penicillin G in a SA practice
- clamoxyl is even worse - in addition will not be in the wound at the time needed

Which are the best?
- Def want something that can treat Staph
- FLuoroquinolones are really good against gram negative and can be very potent around humans- try not to use!

Questions that need to be answered in order to use ABs
- quinolones are the most abuse in vet med!

Do we use Antibiotics?

- Pierre was given amoxicillin but it reoccured
- need to think about staph infection, gram (-)
- he is intact: need to think about prostate - need to think about drugs that can penetrate this
- could be stones since it is recurrent meaning that it could be an uncomplicated urinary infection
- amoxycillin cannot penetrate the prostate, therefore was a bit better but it returned
questions we need to think about when prescribing AB’s
