definition of AML
malignancy of primitive myeloid lineage WBC (myeloblasts) with proliferation in the bone marrow and blood
progresses rapidly - death in 2mo if untreated, approx 20% 3yr survival if treated
classified using the FAB (French-American-British) system into 8 morphological variants with M0-M7
FAB classification of AML
M0 Myeloblastic with no maturation.
M1 Myeloblastic with little maturation.
M2 Myeloblastic with maturation.
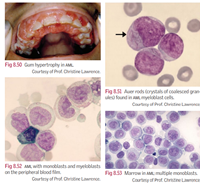
M3 Promyelocytic with coarse cytoplasmic granules. Characteristic Auer rods (crystallisation of granules resembling bundle of sticks or ‘faggots’). Associated with DIC.
M4 Granulocytic and monocytic differentiation (myelomonocytic).
M5 Monoblastic differentiation.
M6 Erythroblastic differentiation.
M7 Megakaryoblastic.
aetiology of AML
myeloblasts are arrested at an early stage in development, with varying cytogenic abnormalities
eg gene mutations and chromosome translocations
undergo malignant transformation and proliferationm with subsesquent replacement of normal marrow elements, bone marrow failure
epidemiology of AML
most common acute leukaemia in adults
1/10000/yr
increased incidence with age
sx of bone marrow failure in AML
anaemia - lethargy, dyspnoea
bleeding - thrombocytopenia, or DIC (DIC in acute promyelocytic leukaemia, a subtype of AML, where there is a release of thromboplastin)
opportunistic/recurrent infections
sx of tissue infiltration - AML
gum swelling or bleeding
CNS involvement - headache, nausea, diplopia
especially with M4 adn M5
signs of bone marrow failure - AML
pallor
cardiac flow murmur
ecchymoses
bleeding
opportunistic or recurrent infections - fever, mouth ulcers, skin infections, PCP
signs of tissue infiltration - AML
skin rash
gum hypertrophy
deposit of leukaemic blasts - may rarely be seen in the eye - (chloroma), tongue and bone (can cause fractures)
hepatosplenomegaly
CNS rare
Ix for AML
blood
- FBC - low Hb, low plt, variable WCC
- high uric acid
- high LDH
- clotting studies
- fibrinogen and D-dimers - when DIC is suspected in M3
blood film - AML blasts may show cytoplasmic granules or Auer rods
bone marrow aspirate or biopsy - hypercellular with >30% blasts (immature cells)
immunophenotypic - Ab against surface Ag to classify lineage of abnormal clones
cytogenics - for dx and prognostic info
immunocytochemistry - myeloblasts granules are +ve for Sudan black, chloroacetate esterase and myeloperoxidase, monoblasts are positive for non-specific and butyrate esterase
associations with AML
can be a long term complication of chemo
myelodysplastic states
radiation
syndromes eg Down’s
