All MSK and Arthritis Flashcards
DIP
PIP
MCP
MTP
Distal Interphalangeal Joint
Proximal Interphagangeal Joint
MCP (knuckle) MetoCarpoPhalangeal
MTP (foot) MetaTarsoPhalangeal
Small bony nodules (osteophytes) at the DIP and PIP joints are characteristic of what?
OA
DIP - Herberden’s nodes
PIP - Bouchard’s nodes
Where do you find Rhematoid nodules on the hands?
MCP
(knuckles)
Deformities of the finger in RhA
(diagram)

Diagram of Tophi (white subcutaneous nodes)
in Gout
- uric acid crystals

Two main features of carpal tunnel syndrome
Median nerve compression
Thenar muscle wasting
rem. flexor retinaculum
Subluxation in the hand and ulnar deviation of the the MCP joints are characteristic of what?
RhA
What is a pannus?
hypertrophied synovium,
containing inflammatory cells that release collagenolytic enzymes
causing loss of bone and cartilage (chronic RhA)
General facts about RhA
Men or Women?
Geographically areas
Low incidence in Afria, high incidence in North America.
3:1 ratio (females >>)
Can disappear in pregnancy due to immune system adaptations to foreign matter.
symmetrical
HLA-DR4 antigen identified.
Hormonal & viral links
RhA nodules characteristics
Made from fibroblasts.
Pinky colour.
Blood supply on the outside only; can become necrotic.
Locations; extensor surfaces of elbows, forearms and hands
RhA on XR - characteristics
White sclerotic changes - spongy bone looks whiter.
Subluxation of MCP
Wrist/ hand displacement
Thumb - Z deformity
RhA diagnostic criteria
morning stiffness >> 60 mins
stiffness after rest
>> six weeks duration
DIP joints spared
Volar subluxation
Swan neck/ boutonniere, guttering between bones
RhA attacks connective tissue (therefore tendinous sheaths); fingers stay in flexion/ extension
Felty’s syndrome (important)
Rare autoimmune disease
Splenomegaly
neutropenia
RhA
Early sign of RhA?
boggy metacarpal joints
Learn the Gold star slide (differences between RhA, OA, and gout)
need image
Tx of gout
Acute; NSAIDs, (+PPIs) or if can’t tolerate then colchicine or steroids.
Chronic; allopurinol or if not tolerated, try febuxostat
Diagram showing MTP joint

Meniscal provocation test



Trendelenberg sign



varus and valgus knees

ankle anatomy diagram

Dermatome to little finger?

Dermatome to middle finger

Dermatome to the thumb

Dermatome to Inner Forearm

Dermatome to Upper inner arm

Dermatome to knee

Dermatome to medial malleolus

Dermatome to dorsum of foot
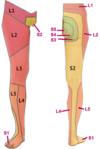
Dermatome to Toes 1-3

Dermatome to Toes 4 and 5; lateral malleolus

