5 - Inflammatory Dermatoses Flashcards
Outline the basic microanatomy of the skin
Epidermis
(between epi and dermis is the basement membrane)
Dermis
- hair follicles
- sebaceous glands
- sweat glands
- collagen
- fibroblasts
- immune cells
- hair follicle + sebaceous gland + erector muscle = pilosebaceous unit
Fat
Fascia
Muscle

Outline the basics of skin histology
In hairy skin, there are hair follicles
Sebaceous glands make sebum which lubricates the hair and contains chemicals which suppress growth of bacteria and fungi
What consititutes the epidermis?
Keratinocytes sit on the basement membrane
- proliferate and move up through epidermis
- differentiate
- make keratin which forms granules
- lose their nuclei
- dead cells at the top
- form stratum corneum (barrier function of skin)
Langherhans Cells = AP cells
Melanocytes = make melanin
Merkel Cells = sensation

What are keratinocytes?
Form the stratum corneum
- dead cells in top layer

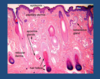
Outline the skin histology of the epidermis
Melanocytes are dark ones at bottom and look vaculated
Top-layer = weave-like structure = stratum corneum

Outline the structure of the stratum corneum
Very important for barrier function of the skin
Defects lead to eczema
Filagrin gene mutation common in eczema patients
- skin is genetically predisposed to be dry
Blocks = keratinocytes
Between cells is made up of lipids and proteins
- one of the proteins is called filagrin

What is atopy?
ATOPY
Tendency to develop hypersensitivity
Give examples of atopic diseases
Eczema
- Atopic eczema is:
- common
- relapsing
- remitting
Asthma
Hayfever
What is The Atopic March?
THE ATOPIC MARCH
People who have atopic diseases tend to develop eczema first early in life (peak at around 2 years of age)
Then they develop food allergies
Then they develop asthma
They then develop rhinitis (hayfever)
What is happening is that the eczema and dry skin is causing them to become sensitised to other environmental allergens

What factors lead to atopic eczema?
INTRINSIC FACTORS
- impaired barrier function of skin (could be due to defective filagrin)
- allows for the extrinsic factors
EXTRINSIC FACTORS
- penetration of allergens into the skin
- irritants such as house-dust mite
- taken into skin
- stimulate immune response
- recruitment of inflammatory cells
- IgE produced
- stimualtes mast-cells to degranulate
- inflammation is perpetuated

What does this photo show?

Palmar Hyperlinearity
- sign of filagrin gene mutation
- the lines on palms and soles are more prominent and easy to see
- therefore, someone with this sign would be more likely to have eczema than someone else with an itchy rash

What do thes photos show?

Infantile atopic eczema
- acute
- skin is red, raw, weepy and may have blisters
- normally in areas where children rub their skin (e.g. face)
- skin on face is more likely to be sensitised to food allergens
- undefined edges

What is atopic dermatitis?

What are the common sites of eczema outbreaks in children and adults?
Sweaty areas predispose to eczema in both children and adults

What does this photo show?

Acute eczema is normally red, weepy and sore
This photo shows chronic eczema
- eczema with lichenification
- lichenification means that the skin markings are much more visible due to lots of scratching of the skin
- lichenification
- erythema
- looks like the skin is becoming thicker
- chronic changes
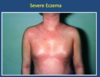
What does this photo show?

Severe Eczema
- erythredermic eczema
- acute eczema (red and weepy) is all over the skin’s surface
- patient is systemically unwell
- should be admitted to hospital
- likely to be staphylococcal infection
- colonises the skin
- perptuates eczema and can also cause infections
What does this photo show?

Eczema herpeticum
- HSV infection occuring in eczematous skin
- HSV spreads all over skin’s surface
- blisters breakdown and form ulcers
- patients should be admitted and treated with acyclovir
- if left untreated, could spread in blood and cause herpes encephalitis in the brain
In ecezema, the skin is not performing its barrier function correctly
- predisposed to infection
- staphylococcus aureus
- also, viral infections such as HSV

List the types of eczema
Seborrhoeic
- overgrowth of yeast with eczema
Allergic contact dermatitis
Discoid
Atopic
What does this photo show?

Seborrhoeic Eczema
- different to atopic
- greasy scale with redness
- dandruff when on scalp
- seborrhoeic eczema on other parts of body
- often occurs in naso-labial folds and scalp
Overgrowth of yeast, but can be primary or secondary to the eczema
Not really itchy but more cosmetically a problem
What does this photo show?

Allergic contact dermatitis
- develop an allergy
- nickel
- perfume
- jewellery
- rubber
- topical treatments
- eye drops
- PPD (black dye) in hair dyes and some henna
- having atopic eczema can predispose to this

What does this photo show?

Discoid eczema
- pattern of eczema
- more in disc shapes scattered around the body
- common in
- elderly
- people who overwash (lipids on skin are washed off)
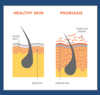
What do these photos show?

Psoriasis
- affects around 3% of the population
- can look similar to eczema
- immune related condition
Presentation:
- plaque (rasied) lesions
- salmon-pink
- silvery scale?
- well-defined lesions
What causes psoriasis?
Genetic susceptibility and an environmental trigger
- then the immune process occurs
- T-cells predominate in the dermis
- stimulates cytokine release (TNF-alpha)
- leads to neutrophils going into epidermis
- overproduction of keratinocytes
- thickening of the epidermis
- top-layer is immature and haven’t lost their nuclei, causing the scaling
Outline the histology of psoriasis
Hyperkeratosis
- thickening of stratum corneum
- scaling of stratum corneum
Parakeratosis
- retention of nuclei in stratum corneum
Acanthosis
- thickening of epidermis
Inflammation
- blackish, inflammatory cells
Dilated blood vessels

What are the common locations of psoriasis?
Scalp
Elbows
Knees
Genital area
However, it can occur anywhere. Also, it is outside of the knees and elbows whereas with eczema, is its on to inside of knees and elbows.

What does this photo show?

Psoriasis soles
Psoriasis vulgaris: soles Well-demarcated, erythematous plaques with thick, yellowish scale and desquamation on sites of pressure arising on the plantar feet; similar lesions were present on the palms.
Can differentiate it from athlete’s foot because it is symmetrical, whereas fungal infections are not often like this. It is also tends to occur in areas of trauma or pressure.
What does this photo show?

Subungal hyperkeratosis
- roughening
- loss of cuticle
- pitting
- build up of keratin
- nail lifts away from nail bed (onycholysis)
Fungal infections in nail:
- yellow crumbly differences
- more common than psoriasis
- normally only affects a few of the nails
What does this photo show?

Dystophic nail and loss of cuticle
What do these photos show?

NAIL PSORIASIS
LHS: Oncholysis
RHS: Oncholysis and pitting
Onycholysis is when a person’s nail or nails detach from the skin underneath.
What do these photos show?

Guttate psoriasis
- rain-drop lesions
- typically in young people after streptococcal infections
- would look for streptococci with nose/throat swab
- can get a lot better if people get lots of infections from tonsils
What does this photo show?

Palmoplantatar pustulosis
- pustules on palms and soles
- tends to just be on hands and feets
- specific genetic predisposition
What do these photos show?

Generalised pustular psoriasis
- pustules (small and white) on inflamed skin
- patient’s are often very unwell
- fever
- malaise
- tachycardia
- need fluid resuscitation
What does this photo show?

Acne
- disorder of the pilosebaceous unit
- usually treated with roaccutane (isotretinoin)
What causes acne formation?
GENETIC AND HORMONAL FACTORS BUT EXACT CAUSES ARE UNKNOWN
Development of Comedone
- due to hyperkeratinsation of the infundibulum of the follicle
- forms keratin plug
Increased sebum production
- androgen stimulation
Overgrowth of of propionbacteria acnes
Inflammation
Cysts forms which then rupture
Lots of dead cells which cause further inflammation
Other Factors:
- Comedone formation
- Genetic predisposition
- Propionibacteria acnes
- Androgenic stimulation

What are the clinical features of acne?
White head = comedone covered in skin
Black head = comedone that is open and dead keratin can be seen
Papule = small inflammatory lesion
Pustule = filled with pus
Nodules = thickened, larger papules

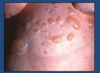
What features does this photo of acne show?

Papules
Closed comedones (whiteheads)
Open comedones (blackheads)
Bad acne can often heal with acne scarring
- better to treat it as early as possible
What does this photo show?

Acne
Treatments:
- topical - lipid-souble and penetrate into sebum
- anti-biotics
- contraceptive pill
- if nothing works, then roaccutane
What does this photo show?
Bullous Pemphigoid
- immunobullous
- autoimmune condition
- generally occurs in the elderly
- make an auto-antibody against a component of the BM
- BM splits
- blisters form
What is important about the basement membrane zone in bullous conditions?
Epidermis is derived from ectoderm
Dermis is derived from mesoderm
There are specific proteins that allow them to bind together
- tonofilaments
- anchoring fibrils
If any are defective, this splits and causes blisters
In bullous pemphigoid, two proteins are the targets of auto-antibodies the cause of the disease:
- BP1-AG1
- BP1-AG2

What does this photo show?

Epidermolysis bullosa
- not an antibody against proteins in BM like bullous pemphigoid
- in epi bullosa, there are defective proteins to begin with
Outline the pathology of bullous pemphigoid
auto-antibodies go to BM zone

What does this photo show?

Bullous pemphigoid
- tense, itchy blisters
- often in elderly
- steroids and other immunosuppressants are given so the skin can recover
What feature of bullous pemphigoid does this photo show?

Tense blisters = bullae
What does this photo show?

Bullous Pemphigoid
- prior to development of blisters, it can look like eczema and urticaria
This female had a severely pruritic generalized eruption that consisted of urticarial, inflammatory plaques, papules and crusted lesions. Originally diagnosed as generalized eczema by the family doctor, the patient was eventually referred to us; and upon close inspection, small vesicles and occasional bullae were seen arising not only in normal but also, and most prominently, in the inflammatory plaques. The diagnosis of bullous pemphigoid, was verified by biopsy and immunofluorescence studies. Note that in contrast to pemphigus vulgaris, where blisters arise exclusively in normal appearing skin, bullous pemphigoidshows blistering in inflammedareas as well; and these blisters are tense.
What do these photos show?

Pempigus vulgaris
- auto-antibodies against desmosomes that connect keratinocytes together in epidermis
- against two proteins desmoglian 1 and 3
- superficial blister which breaks easily and has superifical erosions
- middle-aged people and people of middle-eastern/oriental ethnicities
What are the connections between keratinocytes?
Desmosomes
- these are the targets of autoantibodies in PV

Outline the pathology of pemphigus vulgaris
Line along BM in Pemphigoid
Autoantibody coats around keratinocyte in Pemphigus

What do these photos show?

Pempigus vulgaris
- treated with steroids and immunosuppressants to allow skin to recover
