4.2-Gastric & Peptic Ulcer Disease Flashcards
What are the normal secretory components of the stomach?
- Upper 2/3s; parietal cells secrete HCl and intrinsic factor and chief cells secrete pepsinogen
- Lower 1/3 secretes bicarbonate-rich mucus (mucus cells)+ gastrin from G cels
Name some common symptoms of gastritis and PUD?
- dyspepsia
- anorexia
- nausea/vomiting
- haematemesis; vomiting blood
- melaena; black tarry stools
- GERD
- acid brash
- retrosternal pain
- epigastric abdominal pain
Define gastritis? What is an ulcer and how does it form?
- mucosal inflammation leading to:
- mucosal breakdown leading to
- peptic ulcer disease (duodenal and gastric ulcers)
- mucosal layer breaks down from fissure to erosion to ulcer ie exposed tissue
State the pathogenesis of ulcer disease
- acid
- diet; spicy foods/ coffee
- alcohol
- H. pylori
- NSAIDS
- Zollinger-Ellison syndrome; gastrin secreting tumour of the pancreas
What is Helicobacter pylori?
- major causative factor of PUD
- motile, flagellated ; adheres to gastric mucosa
- spiral cocbacillus
- microaerophilic; o2 is dangerous to it so must survive without it
- urease producing
Describe the importance of the urease reaction in HP?
uses chemotaxis to avoid areas of low pH
- UREASE: neutralises acid in its environment by producing large amounts of urease which breaks down urea to CO2 and NH3
- NH3 then utilises stomach acid to NH4+ ie neutralises the acid
- urease is highly immunogenic ie causes local inflammation which RESULTS IN chronic infection
How does HP damage the stomach/ duodenal linings?
- the ammonia produced to regulate pH is toxic to epithelial cells,
- so are HP proteins EG proteases, vacuolating cytotoxin A (VacA)
- they damage the epithelial cells, disrupts tight junctions and cause apoptosis
-
Cytotoxin associated gene CagA can also cause inflammation+ carcinogenic
*
How can HP be diagnosed?
- UREA BREATH TEST
- Blood test for antibodies
- Stool test; check for an antibody against any antigens of HP
- endoscopy to see if there is a peptic ulcer
Describe the varied phenotype of HP ie how does it affect different people ie manifest itself?
- gastritis only
- intermittent gastric ulcers
- intermittent duodenal ulcers
- gastric cancer
- MALT lymphoma
*
What conditions are associated with the different locations of HP?
1) Antrum only - duodenal ulcer
2) Antrum and body-asymptomatic
3) Body only- gastric ulcer leading to dysplasia in mucosa and cancer
Why do duodenal ulcers result from HP colonising the antrum only?
- Because the antrum is closer to the duodenum
- a large amount of acid goes into the duodenum from the antrum, when it should normally be neutralised at this stage
- Metaplasia occurs in the duodenal lining
What is dysplasia ( in context of gastric ulcers and cancer)?
presence of an abnormal type of tissue which can preceed cancer development stage
Why does HP colonize different areas?
- The localisation of colonisation of HP , which affects the location of the ulcer, depends on the acidity of the stomach ie depends on the individual normal production of acid
- in people producing lots of acid: HP colonises away from acidic area in the pyloric antrum to avoid acidic parietal cells near fundus
- in people producing less acid: could be because of meds eg PPI Omeprazole
- inflammatory response caused by bacteria colonizing near the antrum, induces G cells to secrete gastrin which sitmulates parietal cells in fundus to secrete acid
Why is a bacterium that only colonises gastric mucosa, implicated in duodenal ulceration?
- If HP is in the antrum, near the duodenum,
- then the G cells in the antrum will produce more gastrin; this stimulates HCl production
- Therefore there is increased HCl production from parietal cells into the antrum
- Increased HCl from the antrum passes straight into the duodenum
- causes gastric metaplasia; favourable environment for HP
- therefore allows HP to colonise duodenum ie duodenitis and ulceration
How do NSAIDS cause PUD?
- gastric mucosa protects itself from gastric acid with a layer of mucus, the secretion of which is stimulated by certain prostaglandins
- NSAIDS which are COX1 inhibitors therefore prevent production of these prostaglandins . COX1 inhibitors are worse than COX2 inhibitors
- COX-2 selective anti-inflammatories eg CELECOXIB preferentially inhibit cox-2
this is less essential in the gastric mucosa and roughly halve the risk of NSAID-related gastric ulceration
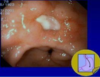
Describe the appearance of a clean gastric ulcer
- nice rolled edges
- mucosa is normal till sloughy base
- flat based pigmented spot ie low rebleeding risks
What is the appearance of a duodenal bulb ulcer?
caused by increased acid secretion

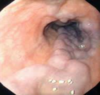
Describe the endoscopic appearance of oesophaeal varices?
- higher up
- normal mucosa on the ends
- varices are lacerated and filled with blood
*
Name 5 techniques of endoscopic management of bleeding?
1) Injection sclerotherapy: inject material into substance to seal it off
2) Diathermy: burning the vessel
3) Variceal ligation: for oesophageal varices; not for ulcer treatment
4) Laser therapy
5) Endoscopic clipping: good for detecting a large vessel that needs to be closed off
-only useful if you can PINPOINT where the bleed is

