12 - ENT Flashcards
Label the tympanic membrane including the quadrants it is split into.

- Pars flaccida at the top
- Pars tensa at the bottom
- Umbo is the tip of the malleus

How do you perform an ear examination?
https: //geekymedics.com/hearing-ear-examination-osce-guide/
- General inspection
- Basic hearing assessment with rubbing tragus
- Weber’s and Rinne’s with 512 Hz
- Palpate the pinna, mastoid process, preauricular area
- Otoscopy with normal ear first and ask about any pain

How is pure tone audiometry performed?
- Wearing headphones they measure what is the quietest sound you can hear 50% of the time at different pitches
- AC measured with headphones, BC measured with headband
- Pure tone threshold is the lowest decibel that the patient hears the pure tone 50% of the time
- May mask the patients other ear by playing a noise into it to stop the cross over problem

How do you read an audiogram?

Red line = right ear
Blue line = left

Why may someone with high frequency hearing loss struggle to comprehend speech?

How may impacted ear wax present and how is it treated?
- Conductive hearing loss, blocked ears or a feeling of fullness, earache, tinnitus, itchiness, vertigo
`- Remove if symptomatic, need to view tympanic membrane or someone needs a mould for a hearing aid
Mx:
- Do not use cotton buds as may become foreign body
- Ear drops for 3-5 days to soften e.g olive/almond oil, NaHCO3 5% (not if ear drum perforation)
- If persists try ear irrigation
- Refer to ENT if after 2 attempts of irrigation and drops no change

How may otitis externa present? (caused by P.Aeruginosa/S.Aureus)
- Acute <3weeks, Chronic >3months
- Diffuse when widespread inflammation of the skin and subdermis
- Localised when infected hair follicle that can become a boil in the ear canal
- Malignant when spreads to surrounding bones e.g mastoid, temporal bones
Symptoms: pain, itch, discharge, hearing loss, red oedematous ear canal, will be painful when touching pinna

How is otitis externa treated?
- Treat pain with analgesic (codeine if severe)
- Warm compress
- Topical acetic acid 2% spray for 7-14 days or topical corticosteroid e.g dexamethasone spray (OTOMIZE)
- If needed oral flucloxacillin for 7 days
- Tell patient to keep ear dry and clean, avoid cotton buds, use hairdryer after swimming or shower

How does acute otitis media present? (Hib, S.Pneumoniae, M.Cattarhalis)
- Most common in children, may hold or rub their ear, or fever, crying, poor feeding, restlessness, cough, rhinorrhoea
- Bulging red, yellow TM with no cone of light
- Risks: second hand smoke, nursery, facial deformities e.g cleft pallate
Complications: recurrence, hearing loss, TM perforation, mastoiditis, meningitis, intracranial abscess, sinus thrombosis, and facial nerve paralysi

How should acute otitis media be managed?
- Check for intracranial complications that need emergency admission e.g mastoid tenderness
- Advise analgesia and explain self limiting 3-7 days
- Delayed or immediate prescription if systemically unwell, amoxicillin or clarithromycin 5-7 days
- Safety net

What are the different ways that you can describe an ear drum perforation?
- Dry or Wet (chronic supparative otitis media)
- Central: if in pars tensa. safer
- Attic/Peripheral: if in pars flaccida. less safe as not under tension
May present with sudden hearing loss, tinnutus, fluid leaking from ear, itchy

How do we manage a tympanic membrane perforation?
- Keep ear very dry and do not put anything in there whilst healing
- Analgesia and warm compress
- Don’t blow nose too hard
- If not healing /chronic supparative after 6-8 weeks refer to ENT for topical steroids, antibiotics and possible surgical tympanoplasty

How does choleasteatoma present and how do we manage it in primary care?
Sac of keratinising squamous epithelium in the pars flaccida that can errode into the middle ear structures
Often asymptomatic to start then foul smelling blood stained discharge. May have retraction pocket with crust/granulation tissue/pearly white/keratin material in upper part of TM
Semi-urgent referral to ENT for audiology assessment and CT. Topical antibiotics before surgical removal

What is this presentation of the eardrum and what is it caused by?
Calcification/scarring of the ear drum due to previous ear infections
Nothing to manage, no symptoms

How does otitis media with effusion (glue ear) present and what are some risk factors of this condition?
- Hearing loss/dulled sounds with occassional ear pain and popping
- May have speech and developmental issues
- Abnormal colour TM (e.g yellow), loss of light reflex, air bubbles, retracted concave TM
Risk Factors: large adenoids, cleft pallate, household smoking, allergic rhinitis, ET dysfunction, Down’s

How is otitis media with effusion managed?
- Observe over 6-12 weeks as may spontaneously resolve with at least two pure tone audiometry tests in this time as well as tympanometry
- Refer to ENT if hearing loss in these tests or symptoms persist after observation period
- ENT may give nasal balloon, hearing aids or do myringotomy and grommet insertion

What is the purpose of the eustachian tube and how can it be blocked?
From the middle ear into post nasal space allowing mucus to clear and equillibriation of pressure when open
Cone of light on TM due to concave TM due to the pressure changes
Blocks: sinusitis, large adenoids, persistent rhinitis, smoking related changes to nasal mucosa

How may otosclerosis present and how is it managed in primary care?
Symptoms: usually bilateral conductive hearing loss, speaking softly, hearing better in noisy surroundings, hearing sounds from within your body, dizziness and balance problems
- Due to abnormal bone growth, especially around stapes and the ossicles may fuse together
Refer for hearing tests and for CT. ENT may give hearing aids or stapedectomy

How does noise related hearing loss present and what does an audiogram of this show?
- May have gradual onset and present with tinnitus, saying ‘what’ a lot, turning up volume on TV
- When exposed to loud noises for too long, e.g working with lawnmowers, stereocilia are damaged
- Permanent!!!! Cannot be reversed, need to prevent by moving away from loud sounds, wearing earmuffs, using noise cancelling earphones

How does Meniere’s disease present and what are some risk factors for this disease?
- Episodes of vertigo, fluctuating sensorineural hearing loss, feeling of fullness in the ear, nystagmus and tinnitus lasting 20 mins-12 hours
- Risks: endolymphatic hydrops, autoimmunity, genetic susceptibility, metabolic disturbances, migraines, viral infection, head trauma
- Will have low to middle frequency sensorineural hearing loss on an audiogram

How can we manage Meniere’s disease in primary care before official diagnose by ENT?
- Admit to hopsital if severe symptoms for IV labyrinth sedatives and fluids
Advice: reassure will clear up in 24 hours but to return if continues for 5-7 days, inform DVLA, don’t operate machinery when dizzy, tell patients to keep their meds always available
N+V: prescribe prochlorperazine or antihistamine/vestibular sedative (cinnarizine, cyclizine, or promethazine teoclate) for 7 days
Prevention: betahistine to reduce frequency and severity of attacks

How does presbyacusis present and how does it show up on audiogram?
Bilateral sensorineural hearing loss often slow onset and in noisy environments at first. Often noticed by other people
Can get tinnitus if gets progressive
Diagnosis of exclusion

How can presbyacusis be managed in primary care after pure tone audiometry?
- Reassure patient it is part of natural aging process
- Communication and environment manipulation e.g speaking face to face
- Hearing aids
- Assistive hearing devices e.g light for doorbell
- Prevent by eating antioxidants, good CVS health, good diabetic control, limiting noise exposure

What is the definition of chronic supparative otitis media?
Chronic inflammation of the middle ear and mastoid cavity, which presents with recurrent ear discharges through a tympanic perforation
Do not swab the ear, refer for ENT assessment
Explain that the hearing loss will return when the perforation has healed

How is mastoiditis managed?
If tympanic membrane is normal it is not mastoiditis as usually follows on from OM
Refer for urgent admission if acute otitis media with mastoid tenderness. Antibiotics or mastoidectomy if abx not working

What hearing loss on an audiogram would a tympanic perforation show?

What can cause referred pain to the ear?
Ear exam normal then examine TMJ, throat, dental hygeine, cervical lymph nodes, general head and neck exam
Take into consideration red flags and risk factors e.g weight loss, voice changes, smoking, chronic alcohol, diabetes
Refer for nasal endoscopy if high suspicion

How do we test for congenital deafness and what are some causes of this?
- Newborn hearing screening AOAE or AABR
Automated otoacoustic emissions
Automated auditory brain stem response
- Causes: infections e.g HSV and rubella, maternal diabetes, low birth weight, preeclampsia, low birth weight, premature birth, alcohol use whilst pregnant

How is congenital deafness managed?
- Aduiology clinic within 4 weeks
- Intervention before 6 months
- Hearing aids from 1 month, cochlear implants from 12 months
- Consider communication method e.g sign language

What can be some difficulties with hearing loss in the following groups:
- Childhood
- Dementia patients
- Visual impairment
- Behaviour and education issues
- Diagnoses issues and impact on confusion
- Difficulties communicating
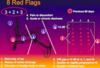
If a patient presents with the folowing red flags, what do you need to consider:
- Unilateral sensorineural hearing loss
- Rhinorrhoea
- Unilateral pulsatile tinnitus
- Recurrent purulent discharge
- Acoustic Neuroma
- Basillar skull fracture
- Vascular cause e.g carotid stenosis, aneurysm
- Choleasteatoma
What is Swimmer’s ear?
Otitis externa
Related to often getting wet

What are some complications of acute otitis media?
- Perforation
- Labrynthitis
- Mastoiditis
What antibiotics should you avoid with ENT issues?
- Tobramycin
- Gentamicin
- Furosemide loop diuretic
Where does the ET tube open into?


What is the retromolar trigone, and where do the thyroid and cricoid cartilages sit?

- Thyroid is shield more superior
- Cricoid sits below

How do you examine the nose in clinic?
- Inspect externally: look for deformities/deviations, lesions e.g BCC
- Inspect nasal cavity: shine light in
- Nasal bone and cartilage palpation: ask about any pain, look for any alignment issues. Look at infraorbital ridges
- Nasal airflow

What are some red flags for a neck lump?

How do you do a neck exam?
- General and Neck Inspection: e.g dyspnea, neck lumps that move with swallowing or tongue protrusion, systemic signs of thyroid pathology, scars, anterior and posterior triangles
- Palpation of lymph nodes and lumps: noting consistency, mobility, tenderness
- Inspect thyroid: see images
- Palpate submandibular gland
- Assess trachea

How do you do a throat exam?
- General inspection e.g swollen lymph nodes
- Lips and gums e.g ulcers, dental hygeine
- Tongue e.g glossitis, candida
- Buccal mucosa, cavity floor and hard palate
- Oropharynx using tongue depressor looking at uvula and tonsils
- Bimanual palpation of glands
- Suggest further exams e.g TMJ, ears, neck

What are the three inputs of the balance system?
- Proprioception (somatosensory)
- Vestibular
- Visual
Sensory inputs cause changes in eye position and limb and trunk position to maintain balance
If any of these are off may feel vertigo (the room spinning)
What is nystagmus and what is the slow and fast phase in jerk nystagmus?
Rapid involuntary movements of the eyes
Jerk nystagmus usually due to inner ear vestibular issues

What are some systems in the body that can cause balance issues?

How does acute sinusitis present?
Usually triggered by URTI and lasts less than 12 weeks
Presence of nasal blockage or nasal discharge with facial pain/pressure (or headache) and/or reduction of the sense of smell
Suspect acute bacterial sinusitis when symptoms last longer than 10 days, discoloured or purulent nasal discharge, severe local pain, fever >38ºC, and deterioration after an initial mild illness
How do we diagnose and manage acute sinusitis in primary care?
Dx: symptoms, tenderness/swelling on palpation of sinuses, anterior rhinoscopy to look for mucosal oedema, polyps, septal deviation
Mx:
- If systemically unwell or infraorbital/intracranial admit to hospital
- Paracetamol/Ibuprofen
- Nasal saline and nasal decongestants
- If >10days with no improvement high-dose nasal corticosteroids 14 days e.g Mometasone BD
- Delayed antibiotic prescription if no improvement after 7 days+10, either Penicillin V or Co-amoxiclav if systemically unwell
- Ask pt to return if not improved in 3 weeks or deteriorates. Could be other cause e.g dental infection

How does chronic sinusitis present and how do we manage it?
- Same symptoms as acute but longer than 12 weeks
- If red flags e.g unilateral blood, neurological/orbital symptoms then refer
Mx:
- Inform pt it may last several months and to control any precipitating illnesses e.g allergic rhinitis, asthma
- Avoid triggers, stop smoking, good dental hygiene, avoid underwater diving
- Nasal irrigation with saline solution
- Nasal steroids up to 3 months if allergic cause e.g fluticasone, mometasone

How do thyroid nodules present and how would you investigate them?
- Solid of fluid filled lumps in the thyroid that are often asymptomatic and found incidentally e.g on US
- If large may be palpable/visible and may compress oesophagus/trachea so trouble swallowing/breathing
- If hyperfunctioning will cause hyperthyroidism e.g weight loss, difficulty sleeping, light periods, anxiety etc
- Ix: TFTs, Thyroid US to see if solid as may be cancerous if solid, fine needle aspiration biopsy, thyroid schintography

How can we manage thyroid nodules?
- Monitor and wait if colloid or hyperplastic nodules
- Surgical removal if compressive symptoms or thyroid adenoma
- Fine needle aspiration if cyst
- Radioactive iodine to shrink hyperplastic nodules or goitre

When should you urgently refer someone down the 2 week wait for a thyroid lump?

How does acute labrynthitis present?
- Often occurs after a URTI
- Presents with sudden, severe onset of vertigo, n+v, hearing loss, tinnutus, unsteady gait, nystagmus
- No hearing loss in vestibular neuritis
- Movement exacerbates not causes vertigo like BPPV
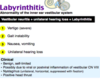
How do we manage acute labrynthitis?
- Assess cranial nerves, gait, nystagmus, hearing
- Urgent referral: sudden unilateral hearing loss/neurological signs/persistent symptoms >1month
- If nothing on the image helps may need surgery e.g myringotomy with effusion clearance

How does allergic rhinitis present and how is it managed?
- Could be seasonal (hayfever), intermittent, occupation
Mx
- Allergen avoidance!!!!
Mild to moderate intermittent:
- either PRN intranasal antihistamines (azelastine) as faster or oral non sedating antihistamine (loratadine or cetirizine)
- consider intranasal chromone (sodium cromoglicate) if above not tolerated
Moderate to severe persistent:
- Regular intranasal corticosteroid when exposed to allergen (mometasone furoate, fluticasone furoate, or fluticasone propionate)
- If nasal congestion intranasal decongestant (ephedrine or xylometazoline) for up to 5–7 days
- If persistent watery rhinorrheoa despite intranasal steroid/oral antihistamine consider intranasal anticholinergic (ipratropium bromide)

When should you refer someone with allergic rhinitis to ENT?
Red flags: unilateral symptoms, blood-stained nasal discharge, recurrent epistaxis, or nasal pain
Persistent symptoms
Septal deviation or nasal obstruction that makes treatment difficult to apply intranasally

How do nasal polpys present?

- Arise from nasal mucosa, usually from middle meatus and are associated with chronic sinusitis/recurrent acute sinusitis, aspirin sensitivity and asthma
- Symptoms: snoring, nasal obstruction, anosmia, watery anterior rhinorrhoea, sneezing, postnasal drainage, dull headaches

How are nasal polyps investigated?
- Nasal exam: yellow-grey colour, look at misting of the speculum for airflow, can get between them and the side wall of the nose
- Rhinoscopy
- Likely to be bilateral, if unilateral with blood stained discharge suggests cancer or foreign body. More likely cancer in Asians
- If in children refer for testing for CF

How are nasal polyps managed?
- Intranasal corticosteroids e.g mometasone and fluticasone, betamethasone
- Oral antihistamines if allergic rhinitis
- Nasal saline irrigation
- LTRA
- Gold standard: functional endoscopic sinus surgery

What are some causes of cervical lymphadenopathy in primary care?
- Infective cause: e.g TB, CMV, EBV, HIV. If persists after 2-4 weeks arrange urgent referral to ENT
- Boils/Abscesses: from infection
- Malignancy: lymphoma, leukaemia, metastasis from lung/stomach
How would you investigate cervical lymphadenopathy in primary care if you are concerned e.g not an infective cause?
- Generalised lymphadenopathy: urgent FBC within 48 hours to look for leukaemia
- Unexplained lymphadenopathy and/or splenomegaly: refer 2 week wait if over 25, refer 48 hours if child or <24 to exclude lymphoma
- >40 with supraclavicular lymphadenopathy: refer 2 week wait for CXR to exclude lung cancer
- >45 with lymphadenopathy/hoarse voice: refer 2 week wait to exclude laryngeal cancer
- Lymphadenopathy and oral ulceration>3 weeks: refer 2 week wait to exclude oral cancer

How does BPPV present and what is the underlying pathology of this condition?
- Repeated transient episodes of vertigo on positional change e.g turning in bed, bending over
- N+V
- Loss of balance

How is BPPV diagnosed and managed?
Dx: Dix-Hallpike manoeuvre showing vertigo and possible nystagmus
Mx:
- Watchful waiting
- Epley manoeuvre
- Brandt- Daroff exercises
- Drug treatment does not help
- Return in 4 weeks if not improved

How do we perform the Dix Hallpike and Epley manoeuvre?
https://www.youtube.com/watch?v=D6qEdlFVxig
What are some symptoms of a deviated nasal septum and what will you see on examination of the nasal cavity?
- Nasal obstruction (difficult to breathe from one nostril)
- Snoring
- Recurrent sinus infections or nose bleeds
- May be congenital or acquired e.g nasal injury in contact sport

How do we manage a deviated nasal septum?
- Take hisotry asking about trauma, impact on life etc
- Symptomatic relief to relieve mucosal oedema e.g nasal decongestants, antihistamines, nasal corticosteroids which take a few weeks to reach maximal effect
- Septoplasty

How does a vestibular migraine present?
- Recurring episodes of vertigo alongside other migraine symptoms lasting 5 minutes to 72 hours. Vertigo is NOT the aura!!!!
- Might have migraines before vertigo for years
- Can rule out other causes with MRIs but can diagnose once at least 5 episodes of vertigo, at least half of these episodes occur with migraines, migraines in the past

How is a vestibular migraine managed?
- Diagnosis of exclusion e.g exclude Meniere’s,
- Mx
- avoid triggers e.g poor sleep, hunger
- usual migraine analgesia e.g ibuprofen and triptans
- prevention with amitriptyline

How does a nasal fracture present and how would you investigate it?
- Symptoms: trauma causing nasal deformity/deviation, bruising, epistaxis, rhinorrhea
- Do nasal exam looking for septal haematoma, facial xray NOT usually performed as diagnosis clinical

How is a nasal fracture managed?
- Analgesia and ice packs
- Closed reduction after 5-7 days so as to allow for swelling to decrease
- Surgical intervention if more complicated

How does vestibulopathy present and what are some of the causes?
Vertigo imbalance, nausea, and vision problems caused by inner ear labyrinth pathology
Patients are at risk of frequent falls
Treatment can focus on inner ear as the cause of imbalance/falls

When an elderly person presents with loss of balance, what are some underlying causes you should consider?

What are some post thyroidectomy complications?
- Hypoparathyroidism: check Ca levels and check for any tingling around mouth
- Bleeding and compartment syndrome which can block airway

What is Samter’s triad?
When an individual has asthma, sinus inflammation with recurring nasal polyps, and sensitivity to aspirin and some other NSAID
They have severe reactions to upper and lower respiratory tract infections

How can you tell the difference between a hypertrophic turbinate and a polp?

What examinations can we do to assess balance?
- Rombergs (loss of proprioception)
- Dix-Hallpike
- Rotary chair test
- Electronystagmography/Videonystagmography

