Written Exam 2 Flashcards
What does the skin do?
- Protective (barrier)
- Minimize water loss
- Prevent entry of pathogens
- UV radiation
- Physical forces
- Sensory
- Body temp regulation
- Produce vitamin D
What layer of the skin are epithelial cells found?
Epidermis
(epi = epi)
Name and describe the layers that make up the skin
- Epidermis (Epi = on top of)
- Dermis
- CT under the epidermis
- Hypodermis (hypo = below)
- CT under the dermis
- Lots of adipose tissue!
- CT under the dermis

Explain the difference between thick skin and thin skin and where each are found
-
Thick skin:
- Found in palm of hands and bottom of feet
- Lots of keratinized epithelium
- thick epidermis
- Varies a lot (differentiation point between thickness of skin)
- smaller dermis
- Found in palm of hands and bottom of feet
-
Thin skin:
- Found everywhere on skin but palms of hands and bottom of feet
- Skinnier epidermis
- Not as much keratinized epithelium
- Thicker dermis

What is skin cancer and why can there be several types?
Cancer = uncontrolled cell growth
How can there be several types?
There is more than one type of cell in the skin
What are the cells found in the epidermis, what type of cancer can be found in each cell type and where they are located?
- Basal Cells = Basal cell carcinoma
- Keratinocytes = squamous cell carconoma (flat c)
- Squamous cells = squamous cell carconoma
-
Melanocytes = melanoma (pigmented moles)
- In basal layer
-
Merkel cells = Merkel cell carcinoma
- In basal layer
-
Langerhans cells = Immune cells in epidermis
- Dendritic cells (stratum spinosum)

What is the function of the tactile cells?
Tactile (Merkel) cells
- located in basal layer throughout. Sensory nerve endings attach to these cells

What is the following layer of the epidermis called and what are the distinct characteristics?

Stratum Basale
(layer base)
- One cell layer thick
- cuboidal or columnar cells
- contain demidesmosomes to attach to CT under
- mitotic cells - stem cells, production of new cells
- contain desmosomes to attach to each other

What is the following layer of the epidermis called and what are the distinct characteristics?
(black arrow)

Stratum spinosum
- No hemidesmosomes (does not attach to CT)
- Has desmosomes (attach to each other)
- Some mitotic cells
- Thicker in thick skin than thin
- Active cells => makes protein (keratin)

Explain the function/process of keratinocytes and where they are located in the epidermis
Keratinocytes in the stratum spinosum
>>>>>
producing keratin
>>>>>
Makes up the intermediate filaments (made of keratin) in the epithelial cells of the skin
(tonofibrils) = special name
Remember: intermediate filaments are involved in intracellular adhesion
Which type of junction involves the intermediate filament?
Desmosomes
= integrins

Explain the components in the following EM slide

Keratinocytes in the stratum spinosum
- Tonofibrils of keratin = dark lines
- intermediate filaments
- Cytoplsamic extensions
- Desmosomes
- electron dense

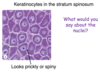
Describe the following slide

Keratinocytes in the stratum spinosum
(looks like a spine = prickly)
- What would you say about the nuclei?
-
Euchromatic = active
- DNA dispersed
-
Euchromatic = active
- Looks prickly or spiny = cytoplasmic extension
What is the following layer of the epidermis called and what are the distinct characteristics?
(black arrow)

Stratum granulosum
- squamous shape
- Only 3 to 5 layers thick
- Cells develop a lipid envelope (water resistance)
- Cytoplasm has Basophilic masses
- Hemotoxylin staining

Explain a summary of the differentiation of cells in the stratum granulosum

-
Cells contain many keratohyaline granules
- Contain several proteins, including profilaggrin
- Granules stain w/hematoxylin = dark color
-
Cells also contin many lamellar grandules
- contain several substances, including lipids
- The nucleus and other organelles degrade and the cells begin to die in this layer

Explain a summary of the keratinization of cells in the stratum granulosum
-
Proflaggrin is proteolysed into multiple filagrin monmers.
- Free filaggrin binds to keratin intermediate filaments, causing aggregation into macrofibrils
- intermediate filaments aligned in tightly packed parallel arrays
- Free filaggrin binds to keratin intermediate filaments, causing aggregation into macrofibrils
-
Lipids and other substances are secreted from lamellar granules
- forming a lipid barrier encircling the cell
- Lipid + filaggrin + keratin matrix = important skin barrier

Explain the end result of keratinization in the stratum granulosum layer of the epithelium
End result of keratinization -> cornified cell
Compressed keratin + filaggrin
-
Contains lipid envelope:
- Prevents abrasion
- Prevents desication
- Protects form infection

What is the following layer of the epidermis called and what are the distinct characteristics?
(black arrow)

Stratum lucidum
- light layer above the stratum granulosum
- ONLY in thick skin
- Cells that lost their organelles
- Contain desmosomes = cells still attached to each other

What are the following structures in this slide?

stratum lucidium = light layer
stratum granulosum = dark layer

What is the following layer of the epidermis called and what are the distinct characteristics?
(black arrow)

Stratum corneum
- Very thick in thick skin and very thin in thin skin
Non nucleated, keratinized cells called squames or cornified cells
- Contains loose desmosomes
- Cells at surface begin to sluff off as the desmosomes break down
- Keratin dust

Where are melanocytes located?
What is the function of melanocytes?
- Melanocytes = dispersed throughout the stratum basale
- Melanin is packaged in small special vesicles called = melanosomes
- Melanocytes have cytoplasmic extensions or dendrites. The melanosomes mature and move to the tip of the dentrite
- The tip of the dendrites with the melanosomes is engulfed by keratinocytes and the melanosomes move towards the nucleus
- Produce melanin and transfer it to keratinocytes
- Tip of the melanocyte gets moved/bit off and goes to the keratinocyte

What is the following cell?

Melanocyte
Can tell it is a melanocyte because of the hollow (clear area)
- Error from the tissue processing
Melanin capping the nucleus of a keratinocyte

Why does melanin accumulate in this supranuclear cap?

Protects DNA from UV radiation
- All skin color has the SAME DENSITY of melanocytes, however there may be LESS MELANIN IN KERATINOCYTES
What are these brown stained cells?
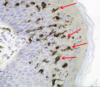
Langerhans Cells
- Immune cells
Type of dendritic cells
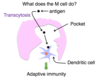
Explain how langerhan cells, or dendritic cells, are involved in immune response
Immune cells
Phagocytize antigen
>>>>>
move to the lymph node
>>>>>>
Present the antigen to lymphocytes
START THE IMMUNE RESPONSE
DEFECTS IN CUTANEOUS BARRIER FUNCTION CAN PREDISPOSE AN INDIVIDUAL TO SKIN DISEASES, SUCH AS ATOPIC DERMATITIS. A GENETIC DEFECT CAUSING THE LOSS OF WHICH OF THE FOLLOWING WOULD MOST LIKELY CONTRIBUTE TO THIS?
Filaggrin
rash development and holes in skin
Because it deals with keratinization and is the cutaneous barrier

What features can be found in the dermis of the skin?
Blood vessels
Connective tissue
Hair
Nerves
Sebaceous and sweat glands
Sensory receptors
What do you notice about the interface between the epidermis and dermis?
What are their functions?

Dermal Papilla = bumps up from the dermis
Epidermal Ridge = Pokes down from the epidermis
Strength - ie reinforce the dermal-epidermal junction
What are the two following layers in the thin skin sample
-
Papillary Layer = dermal papilla - up from dermis
- Fine collagen, elastic fibers with
- MORE CELLS
- Loose CT
- Fine collagen, elastic fibers with
-
Reticular layer = network of CT
- Course collagen, elastic fibers
- LESS CELLS
- Dense Irregular CT
- Course collagen, elastic fibers

What type of collagen is found in the dermis?
Type I = lots in the reticular layer
Type III = Reticular fibers. Lots in the papillary layer (dermis)
Type IV = In the basal lamina/basement membrane (papillary layer = dermis)
Type VII = Anchoring collagen (papillary layer)
Note: Basement membrane is considered part of the dermis
basal lamina = basement membrane = dermis
What are the two types of sensory receptors in the skin?
Nerve Endings
- Not encapsulated
-
Encapsulated (mylinated)
-
Collagen and modified schwann cells
- Schwann cells = form myelin sheath
-
Collagen and modified schwann cells
What is the function of free nerve endings and where are they located?
Free nerve endings = sensory neurons
Location = epidermis
Function: Sense pain, temperature, itching, light pressure (touch)

What is the function of Merkel cells and where are they located?
Location: Scattered throughout basal layer of epidermis which is connected to the
merkel (tactile) disc
Function: Sense light touch
Non-encapsulated = simple nerve ending

What is the function of root hair plexus nerves? Where are they located?
Location: Nerves wrapped around the plexus of a hair
Function: sense hair movement

What are the two types of corpuscles that are found in the dermis and where in the dermis are they located?
-
Meissner corpuscle
- Sits in the dermal papilla
-
Pacinian Corpuscle
- Deeper in the dermis

What is the following feature?

Meissner Corpuscle
- Extremely difficult to see and will be super lucky to find one
- Sits in the dermal papilla
- Unmylinated nerve ending
- Surrounded by modified schwann cells and capsule
- Function: feel shapes, detail
- Location: Hands, fingers, lips, tongue and sole of the feet

What is the following feature and explain function, location, details

Pacinian corpuscle
Very easy to see in a section of your skin
- Location: Deeper in the dermis
- Axon w/modified schwann cells
- Function: Course touch, pressure and vibrations
- Not too many but due to large capusle they can sense when capsule is moved

A 34 year ld female is stung by a bee. She develops urticaria (hives) and pruritus (itchiness). What is going on in the dermis of the skin to cause this reaction?
Mast cells degranulate and release histamine
mast cells are in the skin!!
What causes itching?
Free nerve endings
- Histamine release
- Histamine binds to H1 receptor
- Itching feeling
Explain the anatomy around the hair follicle
-
Arrector pili muscle = smooth muscle
- Body temp. regulation
- Sympathetic nervous system (involuntary)
- Outside in:
- Invagination of the epidermis
-
External rooth sheath
- Sheaths the root of the hair, not involved in the production of the hair
-
Matrix
- Under the sheath
-
Hair pulp, Dermal papilla
- nutrient/blood supply to matrix
- CT with blood vellels

Explain the anatomy of an oblique section of a hair follicle

Oblique section of a hair follicle
- Cells move up and are keratinized to form the hair root and shaft
-
Matrix
- Dividing epithelial cells and melanocytes
- Because hair has color to it
- Epithelial tissue = avascular, cells need nutrients from the dermal papilla
- Dividing epithelial cells and melanocytes
-
Dermal papilla
- CT with blood vessels
- Supplies blood to the hair (to matrix)
- CT with blood vessels

Explain the anatomy of a cross section of a hair follicle

**Do not see matrix here
- Connective tissue sheath
-
Glassy membrane
- Like the basement membrane
-
External root sheath
- Invaginated epidermal cells
-
Internal root sheath
- Comes from the matrix with a softer keratin
- Not from head or skin
- Comes from the matrix with a softer keratin
- Hair (keratinized cells)

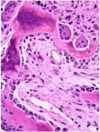
What is the following feature and where are they located?
Why does the feature not stain?

Sebaceous gland
- These are epithelial cells that make up the gland
- Produce: sebum
- Lined with undifferentiated epithelial cell differentiate into sebocytes
- Then lined with Basal lamina
- Outside layer: Connective tissue capusle surrounds the gland
- Location: Face, forehead, scalp
Does not stain: Cytoplasm filled with fat droplets
Sebum = waxy mix of cholesterol and fat that coat the skin and hair

How is sebum secrted into the hair follicle with sebaceous gland?
Holocrine secretion

What type of glands are sebaceous glands?
Branched acini

Name and the following features in the image and where they are located

- Duct opens to surface
- Eccrine sweat gland (All over the body)
- Duct opens to hair follicle
- Apocrine sweat gland (axillary and perineal regions)

What is the following structure?
What are the following features in the structure

Eccrine sweat gland
- Small lumen
- Cuboidal epithelium with underlying myoepithelial cells
- Duct

What is the following structure?
What features make up the structure?

Apocrine sweat gland
- Large lumen
- Cuboidal epithelium with underlying myoepithelial cells

what type of tissue is cartilage?
Connective tissue
What are the types of cartilage and where are they found?

-
Hyaline (blue)
- Articular cartilage (ie. Joints)
-
Fibrocartilage (red)
- Vertebral disks
-
Elastic (purple)
- Ear

What is the following features in the image?

-
Perichondrium
- Peri = around
- chondro = cartilage
-
Hyaline cartilage
- Dark spots inside cartilage = chondrocytes
- cells of cartilage
- Dark spots inside cartilage = chondrocytes

What is the following picture of? name and describe the features of the tissue

Hyaline cartilage
- Very glassy
- Lots of extracellular matrix
- Contains lots of condracytes
Does the extracellular matrix in the perichondrium look the same as the ECM in hyaline cartilage?
Describe the tissues in the cartilage layers

NO
- Perichondrium:
- Dense CT
- Type I collagen
- Hyaline cartilage:
- Type II collagen fibrils
- Lots of ground substance
- forms a gel

Why does the extracellular matrix in hyaline cartilage appear more purple?

Blue + pink = purple
-
Aggrecan = proteoglycans
- Protein + GAG (lots of negatively charged sulfates)
- Proteoglycans!!! Lots of branching (purple in color)
- Protein + GAG (lots of negatively charged sulfates)
-
Hyaluronic acid
- Glycosomino glycan in the ground substance (GAG)
- Blue color
-
Type II collagen
- Fibers = more pink

Why is the extracellular matrix in hyaline cartilage like a gell?

Lots of negatively charged sulfates and lots of water
-
Aggrecan
-
Protein + GAG
- Lots of negatively charged sulfates
- attach/attracted to water molecules
- Lots of negatively charged sulfates
-
Protein + GAG
Becomes a high water content gel

What is the function of the type II collagen and the ground substance in hyaline cartilage?
-
Collagen = gives it tensile strength
- Do not want to rip a part
- Type I = strength
- Type II = lots of strength in cartilage (prevents ripping)
-
Ground substance = makes it resistant to pressure
- want some squishiness
What type of cells are in each of the layers of hyaline cartilage?

-
Perichondrium =
- Fibroblast or fibroblast like cells in the perochondrium
-
Hyaline cartilage =
- chondrocytes in the lacuna (empty space like a lake artifact)

Why does it take a long time to repair damaged cartilage?
- Cartilage is avascular (long time for repair)
- Blood supply is in the perichondrium
-
Chondrocytes have low metabolic activity and limited ability to divide
- pretty static
- Chondrocytes still need nutrients, get it in the perichondrium
Where do new chondrocytes and matrix come from?

fibroblast like cells
>>>>>>
differentiate into chondroblasts
(adding more cartilage on top of other cartilage)
(apositional growth)
Can divide and lay down matrix
(some ability for chondrocytes to divide)
>>>>> Intersititial growth (inside cell)

What is the difference between hyaline, elastic and fibrocartilage?
-
Hyaline
- Type II collagen
- Perichondrium present
-
Elastic
- Type II collagen and elastic fibers
- Perichondrium present
- Ex. epiglotis
-
Fibrocartilage
- Type I and II collagen -> CT very strong
- No perichondrium present
- Ex. intervertebral discs -> super strength

What type of tissue is bone?
Connective
What are the components of bone and function? Cells and extracellular matrix
-
Cells
- Osteoblasts - remodeling
- Osteoclasts - remodeling
- Osteocytes - helps ‘maintain’ matrix
- Bone lining cells
- Osteoprogenitor cells - gives rise to osteoblasts
-
Extracellular matrix = bone matrix
- Fibers
-
Ground substance
- GAGs, proteoglycans, multiadhesive glycoproteins
What type of collagen is in bone?
Type I collagen
Lots of STRENGTH
(tendons, ligaments, bone, skin, sclera, etc)
Explain the fiber arrangement in bone tissue and its major function
- Function: STRENGTH in MULTIPLE directions
- in layers
- The fibers in bone are aligned in parallel, but oriented in different directions
- Called LAMELLAR BONE
- CONCENTRIC LAMELLAE = layers
- Called LAMELLAR BONE

What else gives bone its great strength?
Bone matrix is CALCIFIED
Type I collagen + ground substance = calcification
>>>>>>
Mineralized with hydroxyapatite crystals
Insoluble salt of calcium and phosphorus
= forms a crystal
Explain the structures of ground bone

Ground bone
because bone is so hard you cannot section it without getting ride of the calcium or grinding it down to see the sections
-
Layers of bone matrix
- each of these layers = lamella
- Osteocytes in lacunae (lake)
-
Central canal
- Contains blood supply for osteocytes in the lacunna
- ** Contains no capillaries**
-
Canaliculi
- Little channels between the lacuna in the matrix of the bone
-
osteon
- one circular bone structure

What is the following structure?

Osteocyte in a lacuna
- Dendritic process surrounded by bone matrix
>>>>>
Within the canaliculi

What happens in the canaliculi?
- Osteocytes are encased in mineral matrix that prevents diffusion of substances
- Osteocytes sit in a lacuna
Nutrients: travel from central canal to osteocytes via dendritic process
Wastes: travel from osteocytes to central canal via dentritic process

What type of intracellular communication structure aids with the transfer of nutrients from one osteocyte to another?
Gap junction
What are the types of bone?
Name and describe
-
Lamellar bone
-
Compact bone
- cortical bone = because it generally located on outer edge or cortex of bone
-
Cancellous bone (spongy, trabecular bone)
- Looks spongy and contains trabeculae
-
Compact bone
-
Woven bone
- Occurs during fetal development and bone repair. Then remodels to lamellar bone
- FASTER AND EASIER TO LAY DOWN

Explain the structure of compact bone
Contain osteon
- Contain:
- External circumferential lamellae
- internal circumferential lamallae
- interstitial lamallae
- Osteon
- Centraol canal with blood vessels and nerve

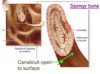
Explain the structure of spongy bone (cancellous or trabecular)
No osteon
- Lamellae = large circles
- Osteocytes in lacuna
-
Canaliculi open to surface
-
Avascular and use canaliculi that open to the surface
- get nutrients from bone marrow
-
Avascular and use canaliculi that open to the surface
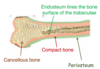
What lines the surface of bone tissue?
-
Endosteum
- Lines surface of trabeculae
-
Periosteum
- lines outside of compact bone
Explain the structure of trabeculae and location of osteoprogenitor cells
-
Endosteum
-
Osteoprogenitor cells or bone lining cells
- Quiesent cells not doing much
- CT layer
-
Osteoprogenitor cells or bone lining cells
-
Periosteum
-
Osteoprogenitor or bone lining cells
- Quiesent cells not doing much
- Dense fibrous CT
-
Osteoprogenitor or bone lining cells
** Dense fibrous CT connected to epithelium via Sharpey’s fibers
- Perforating
- Connects periosteum to the bone

Explain the following structures

Stained section of demineralized bone
- Demineralized by removing the hydroxyapatite crystals
- Calcium phosphate crystals removed to allow for staining

Identify the following structures

Osteocytes
Sharpey’s fibers

Explain the process of bone remodeling
- Resting bone
- Osteocytes or hormones recruite pre-osteoclasts to bone from bone marrow
- Osteoclasts attach to bone and resorbs the bone
- Osteoclasts create a resorption lacuna and release acids and enzymes to remove the bone
- Osteoclast moves/apoptosis
-
Bone lining or osteoprogener cells turn into osteoblasts
- more cube shaped = active
-
Osteoblasts secrete bone matrix
- Lay down osteoid
- Unmineralized bone (Type I collagen that becomes mineralized)
- Lay down osteoid
- Bone mineralizes and traps osteoblasts in matrix to form osteocytes
Identify the following cell types in the tissue sample


Identify the following structures in the image


Identify the following structures in the slide image


Explain the path of osteoclasts movement/remodeling through bone

Identify structures in the following slide/image

What role does osteoblasts and osteoclasts, or bone remodeling, play in the development of osteoporosis?
What exactly is osteoporosis?
Decreased bone mass per unit
volume of anatomical bone
-> Thinning bone over time
Explain the onset of osteoporosis and how bone density changes over time
**Why it is important to build up bone when you are younger so you have more bone you have to break down before getting to a critical level**

Explain a drug commonly used to fight osteoporosis, reaction and its side effects
Bisphosphonate drug inhibits osteoclasts
- Side Effect:
- Osteonecrosis of the jaw = when trauma to the bone (eg. dental surgery) occurs along with continual stress from chewing
- Bisphosphonates disrupt bone remodeling
- Bone has limited capacity for healing
What are the two types of osteogenesis
- Intramembranous ossification
- Endochondral ossification
What are the different shapes of bones?
Long bone (eg. femur)
Short bone (eg. wrist)
Flat bone (eg. skull)
Irregular bone (eg. vertebrae)
What type of ossification does flat bone do for development
Most flat bones develop via intramembranous ossification
- inside a membrane
- Starts out with some kind of membrane
- bone develops in that membrane
Explain the process of Intramembranous Ossification
- Mesenchymal cells in CT membrane or sheet cluster
- Cells differentiate into osteoblasts
- Create an ossification center
- Site where you are making bone
- Osteoblasts secrete osteoid
- Type I collagen and matrix without minerals
- Which then become mineralized
- Osteocyte forms in a lacuna

Explain the slide containing intramembranous ossification

Woven bone (faster)
Newly made
Collagen in multiple directions

What is newly formed bone called?
primary bone or woven bone
NOT LAMELLAR BONE or secondary bone
WOVEN BONE
Collagen in multiple directions, instead of ordered
Because it is faster
- Maturation stage:
- Marrow cavity with blood vessels
-
Immature woven trabeculae
- Collagen fibers oriented randomly
- Mesenchymal cells condense and form the periosteum
-
Remodeling of woven bone >>> Lamellar bone
-
Collagen fibers oriented in parallel
- Formation of cancellous or spongy bone
-
Collagen fibers oriented in parallel

Explain endochondral ossification during fetal development
From cartilage >>>> to bone
DURING FETAL DEVELOPMENT and GROWTH IN LENGTH OF BONE
- Mesenchymal cells condense
- Formation of a chondrocyte (Type II Collagen)
- Hyaline cartilage
- Glassy and do not see fibers
- Forms a perichondrium
- Cartilage deteriorates and turns into bone in the primary ossification center (center long bone)
- Within the primary ossification center)
- Osteoblasts build
- Osteoid and bone is developed (eosinophil)
- Cartilage breaks down (basophilic)
- Initially, form woven bone in the ossification center
- Within the primary ossification center)
SECONDARY OSSIFICATION CENTERS THEN DEVELOP AT THE ENDS OF THE CARTILAGINOUS STRUCTURE
** Woven bone eventually remodels to lamellar bone

Explain how bone grows in width
APPOSITIONAL OR PERIOSTEAL GROWTH
Growth in width or thickening of a bone
- Osteoblast lays down new bone on the surface
- Edge of the bone instead of epiphyseal growth plate

Name and describe the Epiphyseal growth plate zones

-
Zone 1 - Hyaline cartilage
- Resting zone
- Cell type = chondrocytes
-
Zone 2 - Proliferation
- Cells divide
-
Zone 3 - Hypertrophy
- Cells are getting longer
- Compresses the surrounding cartilaginous matrix
-
Zone 4 - Calcification
- Chondrocytes die (apoptosis)
- Because cartilage making is no longer necessary
- Cartilage matrix becomes calcified (more basophilic)
- Chondrocytes die (apoptosis)
-
Zone 5 - Ossification
-
Blood vessels and osteoblasts invade the tissue
- Lays down osteoid
- Creates mineralized bone (eosinophilic)
- Lays down osteoid
-
Blood vessels and osteoblasts invade the tissue

What type of bone will initially be formed at the growth plate?
Woven bone (quick remodeling)
When epiphyseal plate is closed = epiphyseal line and no more cartilage remains in the bone
What occurs when a person has a vitamin D deficiency
= osteomalacia
Calcium does not get absorbed from the gut and then would not allow you to mineralize the bone
- Bone becomes very dull, bowed legs, etc

An excess of growth hormone in adults results in acromegaly. Based on these effects, growth hormone must be increasing:
Periosteal (or appositional) growth
(adult = no more growth at epiphyseal plate)
No more cartilage turning to bone
Instead, Bone grows on the surface

An excess of growth hormone in a child results in gigantism. Based on these effects, growth hormone must be increasing:
Endochondral ossification
cartilage turning to bone
Usually at epiphyseal plate

Explain the features of a synovial (movable) joint

- Joint cavity = creates synovial fluid
- Ligament = connected into bone periosteum to add strength
-
Articular cartilage = Hyaline
- DOES NOT contain periosteum and no perichondrium
-
Joint capsule:
- Make: fibrous layer and synovial membrane

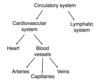
What are the two types of circulatory systems in the body?
What are their divisions
Circulatory system
-
Cardiovascular system
- Heart
- Blood vessels
- Arteries
- Capillaries
- Veins
- Lymphatic system
A person develops a thrombus in their femoral vein. If the clot breaks off, where will it most likely end up?
LUNGS
PULMONARY EMBOLISM
Not going to be able to squeeze through the capillaries in the lungs
- First will travel into right atrium, right ventricle, then into the pulmonary artery into the lungs and get stuck

A person develops a thrombus in their left atrium. If the clot breaks off, where will it most likely end up?
Brain or another organ
STROKE

Name and describe the major layers of the heart

- Endochondrium = Lines inner wall of the heart
-
Myocardium = muscle layer; functions in pumping the blood (contraction)
- Thickest layer
- THICKEST IN LEFT VENTRICLE = TO BODY
- Thickest layer
- Epicardium = Lines the outer wall of the heart

Where is the endocardium in this section of ventricle? What are the layers of the endocardium?
What is contained in each layer?

Endocardium = innermost of heart
-
Myoelastic layer
- Loose CT with smooth muscles
-
Sub-endocardial layer
-
CT with:
- Arteries
- Veins
- Nerves
- Purkinje fibers
-
CT with:

What is the role of the endothelial layer lining the endocardium?

- Acts as a barrier - controls the passage of material between blood and heart tissue
- Provides a nonthrombogenic (non-clot forming) surface
- Prevents clotting
-
Modifies cardiac performance
- Can release different factors that affect the contraction of the myocytes

What is the role of collagen in the endocardium and subendocardium?
Provides SUPPORT

What are the following features?
Describe what they look like and why they are different

Purkinje fibers in the subendocardium of the ventricles
- Do these look a little like cardiac myocytes?
- Tend to be larger than myocytes and a little lighter in color
(have myofibrils but not as many and also contain INTERCALATED DISKS = desmosomes and gap junctions between the Purkinje fibers)

What are Purkinje fibers and why do they look similar to, but different from cardiac myocytes?
Want electrical impulses to get to a lot of myocytes very quickly
- Muscle cells that are specialized for impulses conduction instead of contraction
- Lots of glycogen and mitochondria = not stain as well
- Not many myocytes

Explain the heart conduction system

-
SA node (automaticity = regulatory)
- Generate electrical impulses = contraction
-
AV node
- Slows down impulses to allow atrial contraction before ventricle contraction
-
Bundles of His
- Into the branches and then into the Purkinje fibers that go to the individual myocytes for contraction of ventricles
- Left and right bundle branch
-
Purkinje
- Sends impulses to the myocytes
- Ventricular contraction

Explain what occurs if a person has damage to the endocardium layer of the heart
- If endothelial layer of endocardium intact = no “sticking” of bacteria to the endocardium
-
If endothelial layer is damaged but no bacteria
- Sterile platelet-fibrin nidus forms when platelets adhere to the endothelial layer of the endocardium and then a sterile platelet-fibrin nidus is created
-
If endothelial layer damaged but has bacteria in the blood
- Bacteria binds to the platelet-fibrin nidus and creates a vegetation, potentially causing a death to the patient

While infective endocarditis can occur in the heart chambers, it most commonly occurs on the valves of the heart. Why?
Vegetation often found on the valves of the heart
- Vegetations tend to develop where blood travels from an area of high pressure, through a narrow orifice, into an area of lower pressure
Due to the turbulent flow of the blood around valves causing damage to the endothelium
**All connective tissue in the valves, no muscle

What is the external layer of the heart? and what surrounds the entire heart?
Epicardium
And the surrounding pericardium or pericardial sac

Name and describe the structure/makeup of the epicardium
- Outer surface = Lined with simple squamous or cuboidal layer of mesothelium
- Internal features:
- Autonomic nerve
- Adipocytes or fat cells
- CORONARY BLOOD VESSELS
- bypassed during bypass surgery

Explain the feature that encases the heart
Pericardium or pericardial sac
-
Serous pericardium made up of:
-
Visceral layer
- Mesothelium (right on top of the organ)
-
Parietal layer
- Closed sac
-
Visceral layer
Fluid-filled pericardial cavity (closed sac)
-
Fibrous pericardium = dense CT -> support
- Lots of connective tissue with strength and support to the pericardial sac

If there was a pericardial effusing where fluid built up in the heart. This is caused by fluid building up in which location around the heart?
Between the visceral and parietal layers of the pericardium
- it is where the fluid comes from = serous fluid

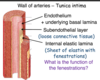
What are the layers of the vascular wall?
Lumen
Tunica intama
Tunica media
Tunica adventitia

What makes up the walls of the tunica intima
- Lumen:
-
Endothelium + underlying basal lamina (basement membrane)
- Simple squamous epithelium
-
Subendothelial layer
- Loose CT
-
Internal elastic lamina
- Sheet of elastin with fenestrations

What is the function of the fenestrations in the tunica intima internal elastic lamina layer
Fenestrations = large holes
-> allows for rapid diffusion through the vessel
Explain the middle layer of an artery wall
TUNICA MEDIA
Circumferentially arranged smooth muscles with:
-
Reticular fibers
- (type III collagen)
-
Proteoglycans and glycoproteins
- (ground substance in ECM)
-
Elastic fibers
- Amount varies - stretch and recoil
External elastic lamina
- Layers of elastic fibers

Explain the outer layer of an artery wall
What type of cells and collagen is found in this layer?
Tunica adventitia or externa
-
Dense irregular connective tissue
-
Collagen and elastin
- Type I collagen = LOTS
-
Collagen and elastin
- Main type of cells
- fibroblasts = elastic fiber production
- Main type of collagen in tunica advantitia
- Type I collagen

What to larger arteries also contain in the tunica advantitia or externa region?
What is the function of this?
VASA VASORUM
- Function = provide blood supply to artery adventitia and media layers
- Contains:
- Arteries
- Veins
- Capillaries
- Nerves

How do systemic arteries differ from systemic veins?
Arteries are subjected to a much higher pressure than veins
- Veins contain:
- One way valves
- Thinner Smooth muscle layer
- Thicker adventitia
- More extensive vasa vasorum

Identify if this is an artery or a vein, identify and describe the layers

Artery
In fact the aorta
Lots of elastic lamina and thick Tunica media

Identify if this is an artery or a vein, identify and describe the layers

Vein
Vena cava
Smaller Tunica media
Thick Tunica Adventitia

What are the types of arteries and their functions
- Conductance vessels
-
Large, elastic arteries (eg. aorta)
- BRANCH
-
Muscular arteries (medium sized arteries)
- BRANCH
-
Large, elastic arteries (eg. aorta)
- Resistance vessels
-
Small arteries and arterioles
- BRANCH
- Capillaries
-
Small arteries and arterioles

Name the feature and describe
What is the function of this type of blood vessel?

Elastic artery
Function: Conduction of blood
ie. helps to store energy generated by the heart’s contraction and helps blood to flow when the heart is relaxing

What is systole and diastole and what is going on with the heart during these two time periods?
-
Systole = Aorta expands or distends
- Facilitated by elastic fibers, limited by collagen fibers
- PRESSURE INCREASES
-
Diastole = Aorta elastic recoil and blood leaves
- Pressure decreases

If the elasticity of the aorta is reduced (eg. increased arterial stiffness possibly from fracture of elastic fibers with aging), what happens to systolic and diastolic pressure?
Systolic pressure = higher
Doesn’t allow for stretch
Diastolic pressure = lower
Doesn’t allow for reduction of area (no recoil)

What is the following feature and describe the detailed structures and function of the tissue

Muscular artery
Very prominent INTERNAL ELASTIC LAMINA
- Endothelial cells
- Internal elastic lamina (prominent)
- Smooth muscle cells
- Predominate constituent of tunic media)
- Adventitia
Function: Same as elastic arteries CONDUCTION OF BLOOD and withstand pressures

What is the following feature and describe the detailed structures and function of the tissue

Small arteries and arterioles
- Function: = resistance vessels
-
Helps determine mean arterial pressure
- Constrict blood vessels = area smaller causing pressure to increase
- All dialated = decrease BP
- All constricted - increase BP
- RIght before the capillaries
- Controls the amount of blood going into the capillary or responsible for the relative blood flow to an organ at any given mean arterial pressure
-
Helps determine mean arterial pressure

What are the following features?


Name and describe the three types of capillaries
-
Continuous = no holes
- Most common
- Contain tight junctions between cells (eg.blood-brain barrier)
-
Fenestrated = small holes
- Allow for proteins, peptides to cross (glands)
-
Sinusoid = Big holes
- Lets RBC through (spleen)

How do material (nutrients, O2, etc.) go from the lumen of the capillary to the interstitial space or visa versa?
Lipid soluble (O2) = diffuse
Some hydrophobic = transcytosis (endo/exo both)
Water and other solutes (excluding proteins) PUSH through junctional complex

What is the advantage of fenestrated vessels?
More rapid, easier exchange of substances like in the kidneys

What is unique about the following sinusoid feature?

Much larger than other capillaries
BOth endothelial layer and basal lamina have large holes
Large enough for cells to get through
What is the following features?

- Small vein
- thin intima with endothelial cells
- thin media
- adventitial blends in
- Small muscular artery

What is the following feature?

Large vein with valve


A. Aorta
Fibrillin = component of elastic fibers
Explain the process of filtration
absorption + lymphatic flow lymphatic vessel
- At the arterial end of a capillary, the sum of the hydrostatic and oncotic forces cause a net movement of material (essentially plasma) form the capillary to the surrounding interstitial tissue
- On the venous end of the capillary, almost all of this material is reabsorbed back into the blood
- The fluid, including proteins, left behind, enters a lymphatic capillary and it ultimately returned to the blood via the lymphatics

Explain the structure of a lymphatic capillary

Endothelial lined cell

Explain what causes the lymph to stain darker
Lymph is rich in proteins and therefore will be more eosinophilic

What happens if filtration is greater than absorption?
such as if a lymph is blocked
Increase protein and water in interstitial space
>>>>>>>>
Non-pitting edema (when more severe)

What is it when the filtration > absorption?
Such as when the venule is is blocked
Increase in hydrostatic pressure increases water in interstitial space
>>>>>>>
pitting edema
Pitting edema = when you press on the skin in the swollen area and the indentation take several seconds to relieve


A. removal of axially lymph nodes from breast cancer surgery

Where does lymph end up?
Larger lymphatic vessels
- Thoracic duct
- Right lymphatic duct
Ultimately to the bloodstream

What are the following features?

LV = lymphatic vessel with very thin walls
V = Venule

What is the following feature pointed out?

Valves in a longitudinal section of lymphatic vessel

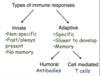
What are the types of immune response and how are they broken down?
-
Innate
- Non-specific
- Fast/always present
- No memory
-
Adaptive
- Specific
- Slower to develop
- Memory
- Humoral = antibodies
- Cell-mediated = T cells
What are cells of the innate immune system?
- Kill virus-infected cells
- Natural killer cells
- Kill worms allergic response Histamine
- Basophil
- Eosinophil
- Mast cells
- Phagocytes kill pathogens
- Macrophage
- Neutrophil
- Antigen Presenting Cells (APC)
-
Monocytes
- Macrophage
- Dendritic cells
-
Monocytes

Within damaged tissue. Which cells act on the injury?
What do these cells do in response?
Mast cells
Macrophages
>>>>>>>>>>>>>>>>>>
Release cytokines (chemical medeators) , chemokines (communication)
these then release histamine, prostaglandins, leukotrienes
>>>>>>>>>>>>>>>>>
Inflammatory mediators
>>>>>>>>>>>>>>>>
Cause the redness and swelling

The immune system can differentiate between self and nonself. How?
Microbes have molecules that are different from hose on our cells
Collectively these different molecules are termed pathogen-associated molecule patterns (PAMPs)

Adaptive immunity is primarily mediated by what type of cell?
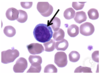
Lymphocytes
You have to look at the surface markers to tell if it is a T cell or a B cell, not seen in the image

Where are lymphoblasts normally located in and what do they differentiate into? and then where do they move to?
- Lymphoblasts
- B cell
- CD4 - T cell precursor
- CD8 - T cell precursor
- NK cells
- Move to the blood in their naive cell form

In the blood B cell, CD4 - T cell precursor, CD8 - T cell precursor, and NK cells in their naive cell form then continue to where and what do they do?
CD4- and CD8- move to Thymus
>>>>>>>>>>>go into>>>>>>
Connective tissue, epithelial, secondary lymphoid organs
>>>>>>>>>>>>>
Wait and look for antigen

Describe Lymphoid tissue and its breakdown
Aggregates of lymphocytes
- Within connective tissue (no capsule)
- Surrounded by a capsule -> lymphoid organ

Describe the breakdown between primary and secondary lymphoid tissue
-
Primary = where immune cells arise (made)
- Bone marrow
- Thymus
-
Secondary = Where immune cells get together and initiate adaptive immunity (lymphocytes)
- Appendix
- Lymph nodes
- Peyer’s patches
- Spleen
- Tonsils

Describe what the thymus is and where does it reside?
Thymus = where T cells mature

Explain the histology of the following slide and state what it is

Thymus
- Contains:
- Capsule = because it is a lymphoid organ (made of CT)
- Septa = dividing the lobule
- Lobule = a lobe with a cortex and medulla
- Cortex = outside of lobule
- Medulla = inside of lobule

WHat type of cells are in the cortex of the thymus?

- Thymocytes (developing T - cells)
-
Cortical thymic epithelial cells (TEC)
- large euchromatic nucleus

Describe the structure of the Thymus and the type of collagen
Lymph node has type III collagen to allow support but Thymus does NOT have this…
Instead, they have
Thymic epithelial cells
These cells are a support network with lots of desmosome processes
Inside the Thymic epithelial = Thymocytes

There is one type of cell that is distinct to the thymus. What is this cell and what layer is it in?
What other cells are in this portion of the thymus?

Hassall Corpuscles
ONLY in the Medulla of the thymus
Medullary Thymic epithelial cells
and Thymocytes

Explain the concept of positive selection in the cortex
- T cell progenitor originated in bone marrow, enters from the blood to the thymus
- Creates Thymocyte
- Proliferation TCR gene rearrangement in the thymus and then express CD4 and CD8 =>
- Creating CD4 and CD8
- It contains both CD4 and CD8 it will then be a double positive thymocyte
- It lacks a T cell receptor (TCR) and CD4 and CD8 co-receptors double negative thymocyte
-
The double positive thymocyte will then either be recognized by MHC or not recognition of MHC (does not occur in thymus)
- If MHC is recognized => presents self-antigen on APC and Thymic epithelial cell (TEC) moves to the medulla
- If MHC is not recognized (95% of them) then the thymocyte dies via apoptosis (neglect)
In the thymus, cortical thymic epithelial cells express a high density of MHC class I and class II molecules associated with self-peptides.
- TCR on a double positive thymocyte binds to an MHC on cortical thymic epithelial cell, the thymocyte moves to the medulla
- If it does not, the thymocyte undergoes apoptosis or dies by neglect

Explain the process of negative selection (occurs in the medulla)
Binds with high affinity to MHC of Professional APC cells (Dendritic cells, Macrophages or less often cortical thymic epithelial cells)
- If there is a high-affinity binding of the thymocyte with CD4, CD8 and TCR then the cell is going to apoptosis
- Gets rid of T cells that would cause an autoimmune response (cell killer cells)
- If there is not a high-affinity binding the surviving double positives -> Matures further to either a:
- CD4 + cell
- CD8+ cell

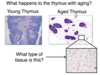
What happens to the thymus with aging?
Loss of thymocytes and gain of adipose tissue
Because of the aging thymus and thymocytes turning into fat cells, they helps to explain why as you get older you are more likely to get sick
Why does the medulla of the thymus stain lighter than the cortex with H&E?
Loss of thymocytes by positive selection in the cortex causes the density of cells to be less in the medulla
(they do not mature into the medulla from the cortex, instead, they undergo apoptosis)

What type of cells are normally present in the nodule of a lymphoid organ?
concentration of B cells

Explain the process of activation of B cells
- APC (Dendritic or macrophage) bind to bacteria and capture antigen => Present bacterial antigen on surface
- MHC with bacterial antigen travels to the lymphoid tissue
- Bind and activate a naive CD4+ T cell
- Activated CD4+ helper T cell created
- Helps activate a naive B cell
- Colonal expansion of B cells, differentiate into plasma cells
- Enter bloodstream and are targeted to the site of inflammation
- Produce antibodies

Explain the activation of cytotoxic T cells
Antigen from virus infected cell or tumor cell binds to MHC I or MHC II on dendritic (APC)
- If MHC I => Bind and activates a naive CD8 T cell
- If MHC II => bind and activate a naive CD4+ T cell
- Helper T cell releases cytokines => leading to a strong CD8+ activation
- Colonal expansion of activated cytotoxic CD8+ t cells
- Functional cytotoxic T cells enter blood stream
- Search and kill virus infected or tumor cells

Explain the structure of a lymph node and what type of cells are located in each region
-
Cortex
- Lymphoid nodules
- B - Cells zone
-
Paracortex
- T - cells zone
-
Medulla
- Plasma cell zone

Explain the flow of lymph in a lymph node
- Afferent lymphatic vessel lymph flows into the
- Subcapsular sinus
- Travels into the trabecular sinus
- In to the medullary sinus (between the medullary cords)
- Out the hilum (efferent lymphatic vessel)

Explain the flow of cells and antigens in lymph into, through and out of the lymph node
lymphocyte, dendritic cell antigen travels into the
afferent lymphatic vessel
Travels through the sinuses
Go back and forth between sinus and parenchyma (functional tissue)
Waiting for antigen







Explain another location where lymphocytes, APCs and antigens can enter the lymph node
THOUGH THE BLOOD
- Comes in through the blood and then high endothelial venule in the paracortex
- is where they enter into the medulla/cortex
- Lymphocytes can now emit into the parenchyma (functional tissue)

What is the following cell and what does it do?

High endothelial venules (HEV’s)
in the paracortex
- Lymphocytes can now emit into the parenchyma
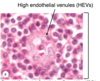
What are the following cells in the figure?

High endothelial venule (HEV’s)
- Lymphocytes crossing the wall
- Endothelial cells
- Cuboidal or columnar
ONLY FOUND IN PARACORTEX OF LYMPH NODE

Where do B cells and T cells that enter a lymph node migrate to?
B cells = cortex (lymphoid nodule or follicle, not active)
T cells = paracortex

In a primary lymphoid nodule, what is occupying it?
Full of naive B cells
NOT ACTIVE

In a secondary lymphoid nodule, what cells are occumpying it?
B cells -> ACTIVE
Outer follicular mantel
Inner germinal center
-> proliferating B cells (turning into plasma cells)
LARGER, MORE EUCHROMATIC CELLS
(darker mantel)



Lymph nodes also contain reticular fibers. What are they?
Lots of reticular fibers (TYPE III COLLAGEN)
- Trabecula

What are the following cells?

Reticular fibers and cells of lymphoid tissues
(Fibroblast-like reticular cells)

What are the following organs?

SPLEEN
(artery and vein)
stomach

What are the features of the spleen?

-
White pulp
- Immune cells (T-cells, B-Cells, APC)
- Red pulp
-
Trabecula
- going in, CT
- Channel before sinus -> now blood vessel
- Capsule
- Trabecular artery and vein

What is the following feature?

White pulp in the spleen
Immune cells
(T-cells, B-cells, macrophages, Dendritic cells)
- Central arteriole
- PALS = mostly T cells
- White pulp = mostly B cells

Explain the following structures

- Marginal zone = macrophages and dendritic cells
- Nodule = B cell zone
- Periarteriolar lymphoid sheath (PALS) = T cell zone

Describe Red pulp

Blood filled sinuses (large capillaries) surrounding splenic cords

Explain the structures in the sinusoid and splenic cords of red pulp
- Sinusoids = splenic sinus = blood vessel
- Splenic cords
-
Reticular tissue = Type III collagen
- Fibroblasts
-
Macrophages
- Phagocytic cells get rid of dead RBC
- Lymphocytes and other blood cells
-
Reticular tissue = Type III collagen

Explain the flow of blood in the white pulp of the spleen
Travels from the
1. Trabecular artery
2. Into central arteriole
3. to the marginal zone sinuses
(termination spot = blind end)

Explain what occurs in the marginal zone sinuses
Cells, antigens, pathogens get into the marginal zone through the sinus
- Antigens, pathogens -> picked up by macrophages, dendritic cells (activate T, B cells)
- The rest continues into the red pulp

Explain the flow of blood in the red pulp of the spleen
Goes from the trabecular artery
into the central arteriole
into the splenic sinus
into the penicillar arterioles
**Blood that enters the red pulp, percolates through and then reenters the blood via the venous sinus

Explain the movement of blood cells into splenic sinusoids
Stave cells = unusual endothelial cells (blood cells can reenter)
Macrophages in spleen (phagocytose older damaged red blood cells)
Reticular fibers help hold in the sinusoid
Space is big enough for white cells and healthy erythrocytes (flexible cells) to pass through











Identify the following structures

Palatine tonsils
- Crypt
- Epithelium

What epithelium overlies the palatine tonsils in the posterior lateral walls of the oral cavity?
What are the dark blue cells?

CT
Stratified squamous epithelium (keratinized)
Dark blue cells = lymphocytes (lots of bacteria in mouth

Identify the structures


What is this a cross section of?

Cross section of ileum - Peyer’s patch = ilium
(lymphoid nodules)
What type of special cells are in the peyer’s patch?
M cell

What does the M cell do?
Antigen enters attaches to the dendritic cell and then activates adaptive immunity
(in the GI track) the largest part of immune response because the food we eat is not sterile
Uses Transcytosis