Presenting complaint Flashcards
Upper abdominal pain ddx
Gastrointestinal
- gastritis
- peptic ulcer
- reflux esophagitis
- pancreatitis
- cancer (gastric, pancreatic)
- Booerhaarve’s disease (esophageal rupture)
- dyspepsia
- irritable bowel syndrome
Pain from nearby areas
- abdominal: central, RUQ pain
- cardiac: e.g. myocardial infarction, pleuritis
- pulmonary: e.g. pneumonia, pleurisy
Right upper abdominal pain ddx
Gall bladder
- biliary colic
- cholecystitis
- cholangitis
Liver
- hepatitis
- hepatomegaly (e.g. liver congestion in right heart failure)
- hemorrhage into hepatic tumour
- trauma
- hepatic or subdiaphragmatic abscess
- Fitz-Hugh-Curtis syndrome (periphepatitis due to PID)
Other gastrointestinal
- appendicitis with high appendix (e.g. pregnancy)
- perforated or penetrating duodenal ulcer
- colon cancer
Pain from nearby areas
- abdominal: epigastric, central, RIF, loin, groin pain
- right lower lobe pneumonia, pleurisy or other lung disease
- subphrenic abscess
- acute pyelonephritis
Left upper abdominal pain ddx
- pancreatitis
- subphrenic abscess
- diverticulitis
- ruptured spleen
- acute pyelonephritis
- leaking aneurysm of the splenic artery
- acute gastric distention
Right iliac fossa pain
Gastrointestinal
- appendicitis
- crohns disease
- inflamed meckels diverticulum
- cholecystitis with low gall bladder
- mesenteric adenitis
- epiploic appendagitis
- colon cancer
- constipation
- irritable bowel syndrome
Reproductive (female)
- ectopic pregnancy
- acute ovarian event (cyst rupture, hemorrhage, torsion)
- Mittelschmerz (ovulation pain mid-cycle)
- Pelvic inflammatory disease
- Endometriosis
Reproductive (male)
- seminal vesiculitis
- undescended testicle pathology
Urinary
- renal colic
- UTI
Pain from nearby areas
- abdominal: RUQ, central, groin pain
- hip pathology
- psoas abscess
- rectus sheath hematoma
- right lower lobe pneumonia
Suprapubic abdominal pain ddx
- urinary retention
- cystitis
- uterine in origin (e.g. PID, fibroid, menstruation)
- origin from RIF and/ or LIF causes
Flank abdominal pain ddx
Renal tract
- infection e.g. pyelonephritis
- obstruction, e.g. renal colic
- renal carcinoma
- renal vein thrombosis
- polycystic kidney disease
- adrenal hemorrhage
Other
- retroperitoneal hemorrhage
- retroperitoneal infection
- vertebral pathology
Referred abdominal pain ddx
- Herpes zoster
- Pneumonia
- Thoracic spine disease
- AMI
- Pericarditis
- Testicular torsion
Abdominal pain hx
- Age
- Pain HX (SOCRATES)
- Associated (GIT history symptoms): focus on nausea, vomiting, bowel motion changes
- Constitutional symptoms
- PMHx (surgery especially)
- Medications
- FHx (colon Ca, diabetes, HTN, IBD)
- SHx (alcohol, travel, occupation)
- Menstrual history (if appropriate)
- Sexual history (if appropriate)
General abdominal pain ddx
- Uraemia
- Hypercalcaemia
- Diabetic ketoacidosis
- Sickle cell disease
- Pb poisoning
Abdominal pain examinations
- Full GIT examination, plus relevant CVS/Resp/renal
- PR
- Vaginal
- Urine analysis
General examinations for abdominal pain
FBC, ESR
Low Hb can show peptic ulcer, malignancy. High WCC indicates infection/inflam. High ESR can indicate Crohn’s or TB.
U&Es
Urea and Creatinine up will provide insight into uraemia.
LFTs
Thinking cholangitis and hepatitis or acute cholecystitis.
Serum amylase
Pancreatitis. Perforated peptic ulcer or bowel infarct can raise also.
MSU
Blood, protein, culture epositive in pyelonephritis. Red cells in ureteric colic. Must think of glomerular disease also.
CXR
Perforated viscus (gas under diaph.) or lower lobar pneumonia.
AXR
Obstruction (dilated loops of bowel). Local ileus (sentinel loop) – pancreatitis, acute appendicitis. Toxic dilation of UC or Crohn’s. Renal calculi. Calcified aorta aneurysm. Radio-opaque gallstones.
US
Abscesses (appendix, diverticular). Fluid in peritonitis. Aortic aneurysm. Ectopic pregnancy. Gallstones. Kidney cysts/tumours.
Specific examinations for abdominal pain
- Blood glucose (diabetic ketoacidosis)
- ABGs (metabolic acidosis)
- Beta HCG (pregnancy)
- ECG (AMI, or electrolyte/K disturbance)
- IVP (Kidney stones)
- CT (aneurys, pancreatitis, malignancy)
- Barium enema (colon Ca, obstructions)
- Colonscopy (tumours, diverticular, colitis)
Constipations differential diagnosis
Congenital
- Hirschsprung’s disease
Obstruction
- Colonic Ca
- Diverticular disease
- Extrinsic compression - Pregnancy, tumours
Anal pain
- Anal fissure
- Perianal abscess
- Haemorrhoids
- Post surg.
Adynamic bowel
- Paralytic ileus
- Ischaemic colitis
- Senility
- Spinal injury
Endocrine
- Diabetic autonomic neuropathy
- Hyperparathyroidism
Drugs
- Codeine
- Morphine
- Atropine
- Tricyclic antidepressants
Other
- IBS
- Diet
- Anxiety
Relevant history constipation
Age
Explore timing, relieving/excacerbating and previous episodes
? Pain Hx (SOCRATES)
Associated (GIT history symptoms)
- Focus on nausea, vomiting, bowel motion changes in past
Constitutional symptoms
PMHx (surgery and trauma especially)
Medication
FHx (colon Ca, diabetes, HTN, IBD)
Menstrual history (if appropriate) Sexual history (if appropriate)
Examinations constipation
- Full GIT examination, plus relevant CVS/Resp/renal
- PR
- Vaginal
- Urine analysis
General investigations for jaundice
FBC, ESR
- Hb low can be anaemia due to malignancy, haemolysis. WCC high from infection (hepatitis, cholangitis). High ESR can be Ca or inflam.
Reticulocyte count
- Haemolysis
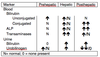
LFTs
- VITAL (see table below)
Viral antibodies
- Viral hepatitis
US
- Gallstones, dilated bilary tree, cirrhosis.
CT
- Ca of pancreas, liver mets.