MSK Flashcards
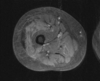
Rice bodies
TB and RA
Diagnosis?

Sever’s
- calcaneal apophysis
Diagnosis?

Bizarre parosteal osteochondromatous proliferation (BPOP)
- also known as Nora lesions
- benign osteochondral lesions which have the appearance similar to an osteochondroma
- typically seen in hands and feet
- continuous with underlying cortext without continuation of the medulla
Concern for septic joint. Sign and indication?

Pneumoarthrogram sign
- Presence of air in the joint excludes a joint effusion and is a normal finding
- No septic joint
T score vs Z score for DEXA
T score = Density relative to young adults
> - 1.0 normal, -1.0 to -2.5 osteopenia, < -2.5 osteoporosis
- False positive - absent normal structures such as laminectomy
- False negative - too much osteophytces, dermal calcifications, metal
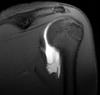
Name 4 types of impingments of the shoulder
- External Primary: abnormal coracoacromial arch
- External Secondary: multidirectional instability “increased glenohumeral volume” with injection
- Internal Posterior Superior: Throwers, posterior superior labrum torn
- Internal Anterior Superior: associated with subscapular damage
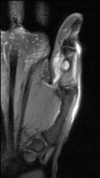
Diagnosis?

Os trigonum syndrome
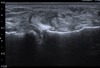
Diagnosis?

Partial Ulnar Collateral Ligament Tear
- Throbwers, anterior bundle of ulnar collateral ligament torn (medial and poster bundles can also be involved)
- T sign
Diagnosis?

Monteggia Fracture
Best radiotracer for osteomyelitis in the spine?
Gallium > WBC scan (In-111)
Diagnosis?

Cortical Desmoid
- misnomer, not a true desmoid
- typically ages 10-15
- repetitive stress injury
- typically seen posterior medial femur at site of medial gastroc attachment or distal adductors
Grading of stress fracture on MRI
Grade 0: Normal
Grade 1: Subtle periosteal edema
Grade 2: Periosteal edema with marrow edema on T2
Grade 3: More edema with changes on T2 and T1
Grade 4: True stress fracture with visible fracture line on MRI or radiograph
Sign and diagnosis?

Double PCL
- Medial meniscus bucket handle tear
- Proves ACL is intact
Pincer type FAI keywords and associations
- Coxa profunda
- Acetabular protusion
- Prominent ischial spine
Asscoiated with os acetabuli, labral tears and early arthritis
Sign and associations?

Looser zones
- wide lucent bands that transverse bone at right anles to the cortex
- Classic locations are femoral neck and pubic rami and have surrounding sclerosis
- Think of osteomalacia and rickets, less common OI
- They are a type of insufficiency fracture
Diagnosis?

Medial epicondylitis
- less common than lateral
- seen in golfers
- common flexor tendon and ulnar nerve may enlarge from chronic injury
Name these 3 wrist factures

- Colles’ fracture - Dorsal angulation
- Smith fracture - Volar angulation
- Barton fracture - involving radial rum, volar is more common
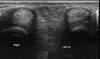
Diagnosis?

Thyroid acropachy (drumstick fingers)
Sign and association?

Arcuate sign
- avulsion of proximal fibula (insertion of arcuate ligament complex)
- 90% are associated with cruciate ligament injury PCL > ACL
Diagnosis?
Transient osteoporosis of the hip
- Ddx for MRI - AVN (has serpigenous dark lines and involves more the subchondral femoral head)
- Bones is lucent on X-ray which looks very different than AVN (sclerotic)
- Regional migratory osteoporosis is similar however affects different joints
DDx Vertebra Plana
MELT
Mets/myeloma
EG
Lymphoma
Trauma/Tb
Diagnosis?

Trevor Disease
- multiple osteochondromas develop at the epiphysis resulting in joint deformity
- most common in ankle and knee
- these point toward the joint
- aka dysplasia epiphysealis hemimelica (DEH)
Diagnosis?

Nail-patella syndrome
- AKA Fong disease and bunch of other names
- Absent/hypoplastic nails from birth, flexion conractures, recurrent knee disloctions, hypoplastic patellas
- Posterior iliac horns (Fong prongs) is pathognomic
- In elbow can see dysplastic radial head, hypoplastic capitellum and lateral epicondyle and prominent medial epicondyle

Has the appearance of a chondroblastoma, but is in adult
Think clear cell chondrosarcoma
Seen near the medial elbow

Epitrochlear Lymphadenopathy
- Classic look for cat-scratch disease
Diagnosis?

Periosteal Osteosarcoma
- Tends to occur in diaphyseal region (rather than metaphyseal)
- Ages 15-25
- Usually no marrow extension
Diagnosis? Potential complication?

Navicular Stress Fracture - seen in runners who run on hard surfaces
- high risk for AVN
Sign and associations

Looser Zones
- Cortical infractions or Milkman lines
- Wide transverse lucencies traversing part way through a bone, usually at right angles to the involved cortex
- Associated with osteomalacia and rickets
- Represent pseudofractures, have sclerotic irregular margins and are often symmetrical
- Commonly located in pubic rami, medial proximal femure, lateral scapula, posterior proximal ulna, ribs
Findings of hyperparathyroidism
- subperiosteal bone resorption of the radial aspect of the 2nd and 3rd fingers
- rugger-jersey spine
- brown tumors
- terminal tuft erosions
Name that ossicle

Cyamella
- located within the popliteus tendon
Bone tumor with fluid-fluid levels DDX
Telangiectatic osteosarcoma, ABC, GCT
Diagnosis?

Dorsal Intercalated Segmental Instability (DISI)
- widening of the SL angle with dorsiflexion of the lunate
DDx?

Osteofibrous dysplasia
- unable to differentiate from adamantinoma, however if anterior bowing present favor OFD
Diagnosis?

Reflex Sympathatic Dystrophy
- a.k.a. Complex reginal pain syndrome and Sudeck atrophy
- Severe osteopenia - looks like unilateral RA, with preserved joint spaces
- Hand and shoulder are most common sites
- usually history of trauma or infection
- 3 phase hot bone scane with intra-articular uptake of tracer due to increased vascularity of synovium

Diagnosis?
Plantaris Rupture
- associated with ACL tears
- only 10% of population has this tendon
- fluid between gastrocnemius and soleus
Skull findings in Paget’s
- Osteolysis circumscripta - large area of osteolysis in the frontal and occiptal bones (lytic phase)
- Cotton wool appearance (mixed phase)
- Thickened sclerotic look affecting inner and outer table (FD favors outer table)
- Tam O’Shanter Sign
- Spine - picture frame sign (extra-credit)
Diagnosis?

Hypertrophic osteoarthropathy
- Primary form is more rare and causes acro-oestolysis
- Secondary form (90%) often due to lung maligancy and causes phaleangeal tuft sclerosis
- Radiographs - long bone metaphyseal and diaphyseal smooth periosteal reaction
- Tc99m MDP - tram track appearance
Findings in adhesive capsulitis
- Decreased glenohumeral volume with injection
- thickened inferior and posterior capsule
- enhancement of the rotator cuff interval
- loss of fat in the rotator cuff interval
Diagnosis and association?

Meniscal ossicle
- ossification of the posterior horn of the medial meniscus
- associated with radial root tears
Types of OI
4 types, in order of most to least common
- least severe and has gracile thin tubular bones and ostepenia
- most severe and typically lethal at the time of or shortely after birth
- most severe that survives into childhood and adulthood
- similar to type 1 except more likely to have basilar skull impression
Sign and association?

Deep Intercondylar Notch Sign
- associated with ACL tears
High risk Stress fractures (7)
- femoral neck (tensile side)
- transverse patellar fracture
- anterior tibial fracture
- 5th metatarsal
- talus
- tarsal navicular
- sesamoid great toe
Diagnosis?

Extensor Carpi Ulnaris Subsheath Injury
Diagnosis?

Osteitis condesans ilii
- benign sclerosis of the ilium adjacent to the SI joint, typically bialteral and triangular in shape
- usually asymptomatic but uncommonly may case lower back pain, often seen in multiparous women
Components of conjoint tendon?
- Biceps femoris tendon
- LCL
Diagnosis?

Little leaguer elbow
- Stress fracture, avulsion or delayed closure of the medial epicondylar apophysis
- usually associated with UCL injury
- valgus overload
Diagnosis?

Scaphoid-Lunate Advanced Collapse (SLAC)
- injury or degeneration (via CPPD) to the S-L ligament
Dupuytren contracture
palmar fibromatosis: progressive condition that causes shortening and thickening of the fibrous tissue of the palmar fascia. Presents as a firm nodularity on the palmar surface of the hand with coalescing cords of soft tissue on the webs and digits.
Compared to a Volkmann ischemic contracture which refers to complex and variable flexion deformity involving distal limbs (typically the wrist and fingers) resulting from fibrosis and contracture of flexor muscles. (results from untreated compartment syndrome)
Intertrochanteric lesions
Lipoma, SBC, FD
Also can think of LMFT

Diagnosis?

Buford complex
- variant in about 1% of population which consists of absent anterior/superior labrum (1-3 o’clock), alogn with a thickend MGHL
Classic association with patellar tendon tear (alta)?
SLE
Can also be seen with elderly, trauma, athletics or RA
Diagnosis?

Pigmented villonodular synovitis
- Radiographs show non-specific features such as joint effusion and bone erosions
- CT and ultrasound can also demonstrate the hypertrophic synovium as a slightly hyperdense/echogenic soft tissue mass.
- MRI is the best approach showing the mass-like synovial proliferation with lobulated margins, with low signal intensity and “blooming” artefact on gradient echo due to hemosiderin deposition.

Diagnosis?

Paget’s of skull
Tam O’Shanter Sign
Diagnosis and association?

Ulnar impaction syndrome
- associated with positive ulnar variance
- distal unla smashes into the lunate, degenerating it and tears up the TFCC
Name Attachments
- Iliac Crest
- ASIS
- AIIC
- Greater trochanter
- Lesser trochanter
- Ischial tuberosity
- Symphysis
- Iliac Crest: Abdominal muscles
- ASIS: Sartorius and TFL
- AIIC: Rectus Femoris
- Greater trochanter: Gluteal muscles
- Lesser trochanter: Iliopsoas
- Ischial tuberosity: Hamstrings
- Symphysis: Adductor group
Diagnosis? Association?

Supracondylar spur (Avian spur)
- can cause compression of median nerve if the Liagment of Struthers smashes it
Diagnosis?

Perthes Disease (LCP)
- white kid age 4-8
Diagnosis?

Volar Intercalated Segmental Instability (VISI)
- volar-flexion of the lunate & scaphoid
- injury to lunotriquetral ligament (ulnar side)
Diagnosis?

Galeazzi Fracture
- Radial shaft fracture with dislocation of the ulna at the DRUJ
Name of this hereditary disorder

Fibrodysplasia ossificans progresiva
- mature ossification within soft tissues, typically starts with sternocleidomastoid followed by shoulder girdle, upper arms, spine and pelvis
- Age of onset is about 5 years of age
- Autosomal dominant
Borders of Quadrilateral Space
- Teres minor
- Teres major
- Medial head of Triceps
- Humerus
- Compression of axillary nerves results in atrophy of teres minor
Diagnosis?

SLAP
- suprior margin and track anterior to posterior, invovles the labrum at the insertion of the long head of the biceps
- When involves biceps anchor (type 4) needs surgical management (biceps tenodesis)
- Not associated with instability

Most likely dx

Glomus tumor
- Hypervascular, T2 bright (compared to GCT tendon which is T2 dark)
Diagnosis and associations?

Carpal Tunnel Syndrome
- Assocation with dialysis, pregnancy, DM, and HYPOthyroidism
- Look for bowing of the flexor retinaculum
Name this sign and what it indicates

Reverse Hamburger Sign
Seen with facet dislocation which can be unilateral or bilateral
Diagnosis?

NF-1
- unilateral, anterior lateral tibial bowing
- may have a psuedofibulararthrosis
- Can be seen in ulna as well

Diagnosis?

Calcaneal stress fracture
- most fractured tarsal bone
- usually intra-articular (75%)
- perpendicular to the trabecular lines
Sign and ddx

Shiny corner sign
- seen in ankylosing spondylitis
- also can see bamboo spine, dagger sign and hatchet sign of humerus (erosion superolateral margin)
Sign and DDx?

Thickened Heel Pad
- Usually <21; if > 2.3 cm in male or 2.15 cm in female then highly suggestive of acromegaly
- DDx MADCOP
- Myxedema, acromegaly, phenytoin therapy (drug), callus, obesity, peripheral edema
Diagnosis?

Osgood-Schlatter Disease
- Adolescents (10-15) who jup and kick- fragmentation + soft tissue swelling
Diagnosis?

Hyperparathyroidism
- First radiographic sign is subperiosteal bone resorption affecting the radial aspects of teh proximal and middle phalanges of the 2nd and 3rd fingers
- Also see subchondral resportion at lateral end of claviles, symphysis pubis and SI joints
- Additional signs, intracortical resorption, terminal tuft erosion (acro-osteolysis), rugger jersey spine, osteopenia, brown tumors, salt and pepper skull, chondrocalcinosis
Progression of red marrow conversion?

Patient with bowel polyps… Diagnosis?

Osteoma
- Often involve jaw in patients with Gardner, however can also involve sinuses and calvarium
- Assocaited with Gardner, but can be seen alone
Diagnosis?

Klippel-Feil Syndrome
- failure of cervical segmentation at multiple levels resulting in short neck and low hairline
- limited cervical motion and increased risk for renal, spinal cord and ear abnormalities
- Associated with Sprengel deformity (tethering of the scapula to the cervical spine by a fibrous band)

Diagnosis?

Bennett Fracture
- Pull of the abductor pollicis longs (APL) tendon is what causes the dorsolateral dislocation
Most common accessory muscle of the ankle?
Peroneus quartus

Diagnosis?

Cartilaginous Bankart
- Periosteum is disrupted, often associated Hill Sach’s fracture

Diagnosis?

Intersection syndrome
- First extensor tendons, intersect the second extensor compartment tendons
- result is ECRB and ECRL tenosynovitis
- Occurs 5 cm proximal to lister’s tubercle
Findings and DDX

Hooked osteophytes at MCP joints
2,3 think CPPD (look for TFCC chondocalcinosis)
2-5 think hemochromatosis (also has uniform joint space loss at all MCP joints, see below)

Ddx?

Osteopoikilosis
- Just a bunch of bone islands distributated around epiphyses, inherited AD
- DDx: Mets
- tend to be keloid formers
Diagnosis? Associations?

Sinus Tarsi Syndrome
- hemorrhage or inflammation of the synovial recess leading to obliteration of the space between the lateral talus and calcaneus
- Associated with rheumatologic disorders and abnormal loading (flat foot in the setting of PTT tear)
Name from left to right and associations

- Peri-lunate dislocation: 60% associated with scaphoid fractures
- Mid-Carpal dislocation: associated with T-L interossesous ligament disruption and triquetral fracture
- Lunate dislocation: happens with dorsal radiolunate ligament injury
Diagnosis?

Lipoma arborescens synovitis
- a rare condition affecting synovial linings of the joints and bursae, with ‘frond like’ depositions of fatty tissue.

Diagnosis?

Sinding-Larsen-Johansson (SLJ)
- Pediatric version of jumper’s knee
- Inferior patella
Patient on longterm dialysis with shoulder hip, wrist and knee pain

Amyloid arthropathy
- joint space is typically preserved until later in the disease process
Diagnosis?

Haglund’s Syndrome/Deformity
- AKA Mulholland deformity
- Prominent posterior superior os calcis, thiceking of the distal achillles tendon
- retrocalcaneal and retro-achilles bursitis

Forearm pain with weakness of extensor muscles and preserved sensation

PIN Syndrome
- AKA deep radial nerve syndrome and supinator syndrome
- result of radial nerve entrapment or compression at the supinator muscle
- MRI shows denervation edema or atrophy of the invovled muscles with sparing of the extensor carpi radialius longus
- Common site of compression is arcade of Frohse at the proximal edge of the supinator
Diagnosis?

Ochronosis or alkaptonuria
- dark urine, build up of homogentisic acid (HGA) from lack of homgentisic oxidase
- broad differential for intervertebral calcification, however if patient’s spine looks like this and they are young then this should come to mind
Name the ankle tendons and imagine their locations!

Diagnosis?

Cubital tunnel syndrome
- Due to accessory anconeus
- Site where the ulnar nerves passes beneath the CT retinaculum also known as epicondylo-olecranon ligament or Osborne’s ligament
Diagnosis?

Juvenile idiopathic arthritis
- Destruction of carpal bones
- premature fusion of growth plates
- widened intercondylar notch (like hemophilic arthropathy)
Diagnosis?

JIA
- Ankylosis of synovial-lined apophyseal joints in the cervical spine may occur at a young age. This leads to a decrease in size of the adjoining vertebral bodies, as well as a decrease in size of the corresponding disc spaces. This most commonly occurs at the C2-C3, and the lower cervical spine is not involed without involvement of the superior cervical spine.

Diagnosis?

Parosteal osteosarcoma
- Bulky tubur loves posterior distal femor (can mimical a cortical desmoid early on)
- Metaphyseal (versus periosteal which is diaphyseal)
*

Primary diagnostic consideration?

Synovial Sarcoma
- T2: mostly hyperintense, the markedly heterogeneous appearance of synovial cell sarcomas on fluid-sensitive sequences results in so-called “triple sign” which is due to areas of necrosis and cystic degeneration with very high signal, relatively high signal soft tissue components and areas of low signal intensity due to dystrophic calcifications and fibrotic bands due to the high tendency of lesions to bleed, there might be areas of fluid-fluid levels known as “bowl of grapes” are seen in up to 10-25% of cases
- Most common malignancy in the foot, ankle and lower extremity in teens/young adults (compared to MFH which is older)
- 90% have translocation of X-18
Diagnosis?
GLAD
- glenolabral articualr disruptions - basically a superficial antetior inferior labral tear
- No instability

Finding and ddx

Widened intercondylar notch
- hemophilic arthritis
- juvenile rheumatoid arthritis
- Tb
Diagnosis?

Subluxation of Biceps Tendon
- Subscapulars tear = medial dislocation of long head of biceps tendon
Diagnosis?

Gamekeeper’s Thumb (Skier)
- Stener lesions - when the adductor tendon aponeurosis gets caught in the torn edges of the UCL

What’s the lesion involving the posterior glenoid?

Kim’s Lesion
- Incompletely avulsed/flattened/mashed posterior-inferior labrum
- Glenoid cartilages and posterior labrum relationship is preserved
Diagnosis?

Adamantinoma
Diagnosis and cause?

Milwaukee Shoulder
- Apocalyptic destruction of the shoulder secondary to the demon mineral hydroxyapatite

Diagnosis?
POLPSA
- Reverse of ALPSA where posterior labrum and posterior scapular periosteum are still intact but stripped from the glenoid
Diagnosis?
Perthes Lesion
- Detachment of anteroinferior labrum (3-6 o’clock) but intact periosteum
- Detached labrum sorta looks like “P”

Diagnosis?

Engelmann’s Disease
- Progressive diaphyseal dysplasia (PDD)
- Fusiform bony enlargement with sclerosis of long bones
- Bilateral, symmetric, hot on bone scan
Name compartments and contents


Name if injury and cause/association?

Calcanial insufficiency avulsion (CIA)
- specific to diabetes
Diagnosis?

Particle Disease
- Most common in non-cemented hips
- Occurs 1-5 years after surgery
- smooth endosteal scalloping distinguishes from infection
- No secondary bone response

Diagnosis?

Gorham Disease
- aka vanishing bone disease
- massive progressive osteolysis with proliferation of thin walled vascular channels
- associated with splenic lesions and soft tissue changes

Name of injury

Pilon fracture
- communited fracture through tibial plafond due to axial loading
Diagnosis?

Pott Disease or tuberculous spondylitis
- spares the disc space until late in the disease
- multi-level involvmement with “skip” involvement
- large paraspinal abscess
- Calcified psoas abscess
- Gibbus deformity
- Brucellosis can mimic this (unpasteurized milk)
Diagnosis and usual imaging findings

SONK (Spontaenous Osteonecrosis of the Knee)
- insufficiency fracture usually involving the medial femoral condyl
- usually unilateral in old lady without history of trauma
DDX

Tumoral calcinosis
- familiar condition with painless periarticular masses caused by hereditary metabolic dysfunction of phosphate regulation
- DDx: HPT, CPPD, myositis ossificans, HADD, tophaceous gout
Most likely Dx

GCT of tendon sheath
- A variant of PVNS
- Intimately associated with tendon sheath
- T1 and T2 low signal, with enhancement
- Differentiated from intramuscular hemangioma by location and by lack of calcifications (phleboliths) on radiographs
Contents of carpal tunnel?


Diagnosis?
Periosteal chondroma (Juxtacortical chondroma)
- lesion in finger of kid, saucerization of the adjacent cortex with sclerotic perisosteal reactoin
Diagnosis? Association?

Kienbocks
- AVN of the lunate - seen in age 20-40
- Associated with negative ulnar variance
- Sclerotic on plan film and radiograph, low signal on T1
Diagnosis?

Giant cell tumor
- Physis must be closed
- Non-sclerotic border
- Abuts the articular surface
- 5% can have pulmonary mets - wide surgical excision is treatment of choice
- most common in the knee
- age 20-30
- can have fluid levels on MRI
- association with ABCs
Diagnosis?
Trigger Finger / Stenosing tenosynovitis
- most commonly shown on U/S
- another common area is flexor hallucis longs tendon around the ankle is patients with os trigonum syndrome
Diagnosis?

March fracture - classically seen in military recruits
Diagnosis?

Kienbock
- AVN carpal lunate
- associated with negative ulnar variance, ages 20-40
Diagnosis?

Sublabral foramen/recess
- Follows contour of the glenoid, smooth margin
- Compared to slap with extends laterally and ratty margin

Diagnosis?

Essex-Lopresti
- Fracture of the radial head + anterior dislocation of the distal radil ulnar joint - rupture of the interosseous membrane
Reducible deformity of joints without articular erosions
SLE or Jaccoud’s arthropathy (ulner deviation)

Diagnosis?

De Quervain’s Tenosynovitis
- Involves first extensor compartment
Diagnosis?

Distal femoral metaphyseal irregularity (cortical desmoid)
peds, scoop-like defect, don’t touch lesion
Diagnosis?
HAGL (humeral avulsion glenohumeral ligament)
- Avulsion of the inferior glenohumar lligament
- J sign when the normal U-shaped inferior glenohumarl recess is retracted away from the humerus, appearing as a J
Axial view over lateral ankle. Diagnosis? Association?
Split peroneus brevis
- C shaped or boomerang shaped with central thinning and partial envelopment of the peroneus longus - alternatively you may see 3 tendons instead of 2
- 80% associated with lateral ligament injury
Diagnosis?

Scheuermann
- 3 adjacent levels with wedging plus thoracic kyphosis > 40 degrees
Diagnosis?

Chondromyxoid fibroma
- least common benign lesion of cartilage
- cortical explanion, eccentrically location, patients younger than 30
- peripheral sclerosis

Diagnosis?

Osteochondritis Dessicans of the capitellum versus Panner’s disease
OCD - in dominant arm of throwers, slightly older patients 12-16 years
PD - Entire capitellum abnormal signal, seen in 5-10 year olds
What is indicated by the arrow?

Pellegrini-Stieda lesions are ossified post-traumatic lesions at (or near) the medial femoral collateral ligament adjacent to the margin of the medial femoral condyle.
Diagnosis?

Freiberg Infraction
- Adolescent girls, can lead to secondary OA
Diagnosis?

ALPSA
- Anterior labral periosteal sleeve avulsion
- Intact periosteum

Diagnosis?

Rolando Fracture
Name sign and diagnosis

Positive Rim sign
Seen in posterior shoulder dislocation
Anteior Inferior Glenohumeral lesions
- GLAD
- Perthes
- ALPSA
- Bankart

Diagnosis?

Osteopathis striata
- linear, paralle, and longitudinal lines in the metaphysis of long bones, doesn’t mean anything
- celary stalk metaphysis

Diagnosis?

Primary synovial chondromatosis
- also known as Reichel syndrome or Reichel-Jones-Henderson syndrome, is a benign monoarticular disorder of unknown origin that is characterized by synovial metaplasia and proliferation resulting in multiple intra-articular cartilaginous loose bodies of relatively similar size, not all of which are ossified.
- Greater in number than in secondary which results from osteoarthrosis or trauma

Diagnosis?

Diabetic myonecrosis
- almost always involves the thigh (80%) or calf (20%)
- marked edema with enhacment and irregular regions of muscle necrosis
Diagnosis?

Osteoblastoma
- Basically an osteoid osteoma > 2cm
- Seen in patients less than 30
- Most common in posterior elements of spine
Diagnosis?

Anterolateral impingement syndrome
- MRI finding is meniscoid mass in the lateral gutter of the ankle
- Injury to ATFL and TFL can cause lateral instability and chronic synovial inflammation
Diagnosis?

Scahoid Non-Union Advanced Collapse
- occurs with a scaphoid fracture
- develop degenerative changes at the radioscaphoid joint
Ddx

Tuberculous dactylitis
- Can have the apperance of an expansile diaphyseal lesion of the digit
- Ddx: syphylitic dacylitis, leukemia, also kinda reminiscent of Macrodystrophia lipomatosa
Diagnosis?

Lateral epicondylitis
- more common than medial, radial CLC complex tear and extensor tendon injury
- seen in tennis players
Diagnosis?

Kohlers
- Tarsal navicular osteonecrosis
- Boys 4-6