Dermatopathology Flashcards
Oculocutaneous albinism, retained visual acuity, immunodeficiency, early dementia
Chediak-Higashi syndrome
- Presence of giant lysosome-related organelles (melanosomes, platelet-dense granules, neutrophil granules)
Disorders with complete absence of melanocytes (3)
- Vitiligo
- Piebaldism
- Waardenburg syndrome
Decreased visual acuity
Lung and GI problems
Absence of dense bodies within platelets
AlbinismHermansky Pudlak syndrome
Hermansky Pudlak syndrome
Absence of stage III/IV melanosomes
Photophobia WITH decreased visual acuity
NO dementia
Albinism
Oculocutaneous albinism
Melanocytes with an INCREASED number of normal-sized melanosomes
Silvery-grey hair
Type 1 has neurologic impairment
Type 2 requires HSCT
Griscelli syndrome
Newborn with clustered vesicles in an arcuate and polycyclic array
What type of EB is this?
EB simplex, Dowling-Meara (EBS-DM) subtype
- Split seen within basal keratinocytes
- Clumping of tonofilaments within keratinocytes’ cytoplasm
What type of EB shows absence of anchoring fibrils due to collagen VII defect?
Dystrophic epidermolysis bullosa (DEB)
What type of EB shows perinuclear stellate inclusions?
Autosomal dominant EB
Reduced number of hemidesmosoms is seen in what type of EB?
Junctional EB
Ziehl-Neelson stain is used to identify what type of bacteria?
Acid-fast bacteria (i.e., mycobacteria)
PCT may have identical histopathologic features to what EB? What type of collagen is targeted in that form of EB?
What findings on DIF can help differentiate the two conditions?
What are the various porphyrin abnormalities in PCT? (3)
(Non-inflammatory) EB acquisita (autoantibodies against type VII collagen)
- DIF for PCT shows perivascular IgG > IgM and complement in the upper dermis
- DIF for EBA shows linear BMZ deposition
- In PCT, there is elevated urine, stool, and serum uroporphyrin.

What type of EB is this?
On electron microscopy, what cytological structures would be absent in the specimen?
What gene mutation is present?
Recessive dystrophic EB (RDEB)
Absence of anchoring fibrils
- Compound heterozygous mutation within the COL7A1 gene, leading to a truncated collagen VII protein that in most cases is nonfunctional

Absence of anchoring filaments, hemidesmosomes, and sub-basal dense plates is seen in what type of EB?
Herlitz subtype of junctional epidermolysis bullosa (JEB)
- Anchoring fibrils are still present in JEB probably accounting for less severe scarring compared with RDEB
Multiple sclerotic fibromas (storiform arrangement of thickened collagen bundles with interspersed spindled cells) are associated with what disease?
What cancers are associated? (2)

Cowden disease
- Autosomal dominant mutation of PTEN gene
- Oral papillomas, trichilemmomas, acral keratosis, sclerotic fibromas
- Benign and malignant breast and thyroid tumors
- GI polyps, skeletal abnormalities
What syndrome is associated with acrochordons, multiple fibrofolliculomas, and trichodiscomas?
What is the genetic mutation?
What cancer is associated? What lung finding may occur?
Birt-Hogg-Dube (BHD) syndrome
Mutation in BHD gene
Associated with renal cell carcinoma and pneumothorax
Gardner syndrome is caused by what genetic mutation?
What are the three skin findings of this syndrome?
APC gene
Epidermoid cysts, osteomas, desmoid tumors
Associated with colorectal adenocarcinoma
What CD is “langerin”?
What is this a marker of?
CD207
Marker of Birbeck granules
What is the best tissue sample for transmission electron microscopy when evaluating for an inherited blistering disease?
A clinically induced blister at the time of biopsy.
Pretibial myxedema histology
Increased mucin within the upper dermis that separates collagen bundles.
The overlying epidermis may demonstrate acanthosis, papillomatosis, and hyperkeratosis.

Muir-Torre syndrome is associated with mutations in which mismatch repair genes? (4)
25% of patients will have what type of skin cancer?
>60% of patients will have what internal malignancy?
- Caused by mutations in mismatch repair genes including MLH1, MSH2, MSH6, and PMS2
- Twenty-five percent of patients with MTS also have keratoacanthomas
- More than 60% of patients will have associated colorectal adenocarcinoma
KRT1 and KRT10 mutations cause what skin disease?
Epidermolytic ichthyosis, in which the pathology is not characterized by acantholysis but rather epidermolytic hyperkeratosis
What gene mutation and organelle is involved in Darier disease (keratosis follicularis)?
What gene mutation and organelle is involved in Hailey-Hailey disease (familial benign chronic pemphigus)?
- Darier disease (keratosis follicularis) → ATP2A2 mutation, encoding the endoplasmic reticulum Ca2+ ATPase
- Hailey-Hailey disease (familial benign chronic pemphigus) → ATP2C1 gene, which encodes the Golgi-associated Ca2+ ATPase
Think of the disease names, mutations, and organelles involved in ALPHABETICAL order. And the organelles involved are just one letter away from the first letter of the name!!
You are called by the neurology team to perform a skin biopsy for the workup of cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. You perform a 4-mm punch biopsy of the arm.
In what medium do you place the specimen?
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is a neurologic disorder caused by mutations in NOTCH3. Patients with CADASIL have migraines, recurrent strokes, and progressive dementia. Transmission electron microscopy (TEM) of a skin biopsy is the gold standard to detect pathologic findings.
Placing the skin specimen in the correct medium, glutaraldehyde for TEM, is critical for accurate diagnosis.
What media should be used for preservation of gout crystals or for fat immunostaining?
Alcohol
What media should be used for immunofluorescence studies? (2)
Michel transport medium or normal saline
EBS with pyloric atresia (EBS-PA) is caused by what genetic mutation?
Mutations in PLEC1 leading to a defective plectin 1 protein
The split described is intraepidermal, which is characteristic of epidermolysis bullosa simplex (EBS).
Junctional epidermolysis bullosa (JEB) with pyloric atresia is caused by what genetic mutation?
The split is within the lamina lucida.
Ectodermal dysplasia skin fragility syndrome can be caused by what genetic defect?
PKP1 gene defects lead to dysfunctional plakophilin 1 and ectodermal dysplasia skin fragility syndrome.
In addition to the clinical findings in the Figure, you see granulation tissue around the mouth, the nape of the neck, and fingernails.

Excessive granulation tissue is a characteristic finding of the Herlitz subtype of junctional epidermolysis bullosa (JEB). This feature is not seen in other inherited epidermolysis bullosa disorders. JEB has a cleavage plane in the lamina lucida.
A 65-year-old man has a pink papule on the right side of the abdomen that has been slowly enlarging over one year. A shave biopsy is performed, and the histopathologic findings are shown (Figure).

Fibroepithelioma of Pinkus (FeP) is an uncommon follicular neoplasm that clinically presents as a fleshy pink papule or small plaque, typically on the trunk.
Like BCC, the majority of FeP cases demonstrate diffuse expression of the proto-oncogene Bcl-2 as well as androgen receptor.
The majority of trichoblastomas demonstrate peripheral expression of _____ and absence of _____ receptor and stromal _____expression.
The majority of trichoblastomas demonstrate peripheral expression of Bcl-2 and absence of androgen receptor and stromal CD34 expression.
Lacazia loboi can be identified using what fungal stain?
Gomori methenamine silver
A 50-year-old man comes to the office for evaluation of 2- to 5-mm papules on the face and neck. A biopsy of a characteristic lesion is performed (Figure).
Which three of the following options are most likely associated with this disorder?

Histopathologic examination demonstrates a fibrofolliculoma, characterized by epithelial strands extending from the undersurface of the epidermis into the underlying dermis with follicular differentiation and a surrounding fibroblast-rich sclerotic stroma.
This may be associated with Birt-Hogg-Dube (BHD) syndrome, which is caused by a mutation in the BHD gene. Renal cell carcinoma and spontaneous pneumothoraces are strongly associated with BHD syndrome.

Immunofluorescence antigenic mapping is an effective technique for the diagnosis of epidermolysis bullosa (EB). Immunomapping with antibodies to BPAg1 and collagen IV allows for differentiation between the major types of EB.
In junctional EB, where do BPAg1 and collagen IV localize to - the roof or the floor?
What about in EBS?
What about dystrophic EB?
Type IV collagen is present in the lamina densa of the basement membrane zone, whereas BPAg1 localizes to the hemidesmosomes of basal keratinocytes. The split in junctional EB is in the lamina lucida, which is below the hemidesmosomes and above the lamina densa. Therefore, BPAg1 would localize to the roof, whereas collagen IV would localize to the floor.
In epidermolysis bullosa simplex, both antigens localize to the floor. In dystrophic epidermolysis bullosa, both antigens localize to the roof.
An 18-year-old woman has multiple slowly growing papules on her face, including her cheeks and forehead. A biopsy showed a proliferation of basaloid cells forming multiple small nests, lobules, and small folliculocystic structures containing keratin material. No significant cytologic atypia, mitotic activity, or infiltrative features were identified.
What is the most likely diagnosis for this tumor?
The histologic findings describe a benign follicular neoplasm composed of basaloid cells forming small nests, lobules, and folliculocystic structures, findings typical of trichoepithelioma.
_____ is the most common drug-induced cause of pemphigus vulgaris.
Penicillamine
What is pseudoepitheliomatous hyperplasia (PEH)?
Epidermal acanthosis, papillomatosis, and hyperkeratosis that can mimic squamous cell carcinoma

True or false: a three-week course of systemic steroids will not affect DIF results.
Deposited immunoglobulin (Ig) must undergo several half-lives (21 days for IgG) to clear completely. As such, a short course of less than 4 weeks of systemic steroids will likely not affect direct immunofluorescence (DIF) test results.
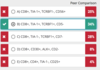
____ and ____ stains are useful for metastatic small cell carcinomas of the lung, as they are typically positive for both of these markers.
_____ and _____ are the best stains for confirming the diagnosis of a metastatic adenocarcinoma of gastrointestinal tract origin, especially lower gastrointestinal tumors, which are usually positive for both of these markers.
CK7 and TTF1 stains are useful for metastatic small cell carcinomas of the lung, as they are typically positive for both of these markers.
CDX2 and CK20 are the best stains for confirming the diagnosis of a metastatic adenocarcinoma of gastrointestinal tract origin, especially lower gastrointestinal tumors, which are usually positive for both of these markers.
Is dermatitis herpetiformis positive or negative on IIF? What about PCT?
Both DH and PCT are IIF-negative.
What is the DIF pattern of PCT?
IgG perivascular “donut” like accentuation and increased signal along the basement membrane zone (BMZ)
What are the optimal location and timing for immunofluorescence testing of discoid lupus erythematosus?
Lesional skin more than 4 to 6 weeks old
Lesional skin is the preferred site to look for immunoreactants in discoid lupus erythematosus (DLE). Deposition of the classic granular band of immunoreactants takes some time and biopsies of lesions less than 4 to 6 weeks old may yield false-negative results.
In bullous pemphigoid and EBA on salt-split skin, do the antibodies bind to the epidermal or dermal side of the salt-split skin? Are the autoantibodies to components of the hemidesmosomes or the anchoring fibrils?
- BP → linear deposition of IgG to the epidermal side (Ab against components of hemidesmosomes)
- EBA → dermal side of salt split skin (Ab against anchoring fibrils)
What are the most common underlying neoplasms associated with paraneoplastic pemphigus?
The most commonly associated neoplasms are non-Hodgkin lymphoma (40%), chronic lymphocytic leukemia (30%), Castleman disease (10%), malignant and benign thymomas (6%), sarcomas (6%), and Waldenström macroglobulinemia (6%).
Figures 1 and 2 show patient skin (left) and normal control skin (right) incubated with mouse anti-human laminin 332 (beta chain).
What is the diagnosis?

In the normal human skin (Figure 1), there is linear deposition of anti-human laminin332 to endogenous laminin332 along the basement membrane. In the patient’s skin, there is some background artifact staining of the epidermis and stratum corneum but linear staining at the basement membrane is not seen, indicating an absence of endogenous laminin332 and the diagnosis of junctional epidermolysis bullosa, Herlitz type.
In cicatricial pemphigoid, whether the autoantibody is laminin332 or BPAg2, endogenous laminin332 is present and binding of an exogenous incubated anti-laminin332 antibody will be detectable.
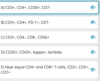
What is the expected immunophenotype of Merkel cell carcinoma?

CK20+ (often exhibiting perinuclear dot-like pattern of positivity) and importantly, TTF-1-negative.
A 55-year-old woman develops an erythematous nodule on the right lower eyelid (Figure).
Which two of the following immunohistochemical studies would be positive in the tumor cells shown?
Both adipophilin and factor XIIIa (clone AC-1A1) would be positive in this sebaceous carcinoma.
Adipophilin is a cytoplasmic marker
AC-1A1 mouse monoclonal antibody for factor XIIIa has been shown to highlight the nuclei of sebaceous cells
A 68-year-old man has an erythematous patch on his foot as shown (Figure).
What is the best diagnosis?

Kaposi sarcoma
Histologically, these tumors show a spindle cell proliferation with abundant irregular vascular spaces containing lymphocytes. A promontory sign (a small vessel protruding into an abnormal vascular space) can be seen. Plasma cells are often evident. Detection of HHV8 latent nuclear antigen on immunohistochemistry is often a helpful tool.
A 30-year-old man has a 1- to 2-cm papule on his upper arm, which he reported as swelling and changing color from blue to yellow.
What is the best diagnosis?

Targetoid hemangioma
Histologically they consist of ectatic vascular channels lined by ‘hobnail’ endothelial cells in the upper dermis. In the deep dermis, the vessels are small, dissect through collagen bundles, and are associated with hemosiderin. Fibrin thrombi can be present in the superficial vessels.
What constitutes “positivity” for PD-L1 by immunohistochemical studies?
PD-L1 positivity is defined as “complete membranous positivity in the tumor cells” (Figure).

What is the alternative name for epithelioid hemangioma?
What is the treatment?

Angiolymphoid hyperplasia with eosinophilia (ALHE)
Histologic examination shows a dermal blood vessel proliferation with a lymphocytic inflammatory infiltrate containing eosinophils. The endothelial cells are large and epithelioid but are otherwise not atypical.
Surgical excision is generally required
A 57-year-old woman comes to you with a 3-cm pruritic nodule on her neck (Figure).
What is the most common therapeutic intervention for this lesion?
Angiolymphoid hyperplasia with eosinophilia (ALHE)
Histologically ALHE shows a well-circumscribed proliferation of blood vessels lined by plump endothelial cells with large nuclei and abundant eosinophilic cytoplasm. An associated stromal inflammatory infiltrate consisting of lymphocytes and scattered eosinophils is also identified. Surgical excision is the most common therapeutic intervention reported.
A 65-year-old patient with history of non-Hodgkin lymphoma, status post recent allogeneic bone marrow transplantation, develops widespread pruritic crusted and hyperkeratotic lesions. A skin biopsy was performed (Figure).
What is the diagnosis?
What do the arrows point out?
Norwegian (crusted or keratotic) scabies
Histologically, they present as massive orthokeratosis and parakeratosis with mites in all stages, psoriasiform hyperplasia, focal spongiosis, and exocytosis of neutrophils and eosinophils. Sometimes intraepidermal microabscesses are seen. The dermis demonstrates a superficial and deep infiltrate of chronic inflammatory cells with interstitial eosinophils.
The presence of egg case remnants, which appear similar to pigtails, can be a helpful clue.
A 53-year-old woman with a history of hepatitis C comes to you with a pruritic rash on the dorsal aspect of her feet (Figures A-C).

Necrolytic acral erythema
The histologic findings include psoriasiform hyperplasia with papillomatosis and dyskeratotic keratinocytes in the clinical setting of a psoriasiform plaque on the dorsal foot of a patient with history of hepatitis C. These findings are most consistent with necrolytic acral erythema.

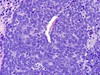
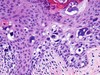
A 64-year-old woman comes to clinic with a 1-year history of infiltrative grouped lesions on the left cheek and lateral eyebrows. A biopsy is performed; the histopathologic features are shown in the images below.

Folliculotropic mycosis fungoides
The low-power image shows a dense perifollicular and intrafollicular lymphocytic infiltrate (folliculotropism). The high-power image shows mucin within a follicle (follicular mucinosis). These findings are compatible with folliculotropic mycosis fungoides (FMF).

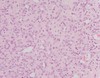
A 10-year-old girl comes to you with multiple yellowish papules on the lateral neck and antecubital fossae. A skin biopsy is performed (Figures A and B). Von-Kossa and Verhoeff-von Gieson stains highlighted calcified and fragmented elastic fibers in the dermis.


A middle-aged man with human immunodeficiency virus has numerous brown macules on the trunk. He feels well otherwise but is bothered by the appearance. The eruption has not responded to topical selenium sulfide lotion or the application of imidazole cream. A biopsy of one of the macules was performed (Figure).
Which of the following is the best diagnosis?

Acquired epidermodysplasia verruciformis occurs in patients with HIV as well as other types of immunodeficiency and may mimic pityriasis versicolor on clinical examination. Biopsy reveals large pale keratinocytes in the granular and spinous layers. There can be a prominent perinuclear halo. Keratohyaline granules of various shapes and sizes can be encountered.
A 37-year-old African-American woman with a history of systemic lupus erythematosus on hemodialysis developed nonhealing ulcers on the buttocks three months ago. The image obtained is shown. Clinical examination reveals well-demarcated ulcerations with granulation tissue and undermined edges. The patient denies any fever or chills and overall feels well. Tissue culture for bacteria is negative. A biopsy was performed. The findings are shown in the second image obtained.
What is the most likely cause of the patient’s ulceration?

Cytomegalovirus (CMV) vasculitis
Secondary vasculitis in lupus can be due to medications or infections. The histopathology image demonstrates characteristic cytomegalovirus (CMV) inclusions (owl’s eye nuclei) in the vascular endothelium (secondary vasculitis) (B).
What is Rowell syndrome?
Rowell syndrome is characterized by erythema multiforme-like lesions in systemic lupus, typically in middle-aged women.

An 85-year-old man is being evaluated for a rapidly growing red nodule on his chest. He otherwise feels well. A biopsy reveals neoplastic cells with hyperchromatic nuclei. Staining with cytokeratin 20 reveals the pattern shown (Figure).
Which of the following is the best diagnosis?

Merkel cell carcinoma
Merkel cell carcinoma presents as a dermal or subcutaneous tumor composed of neoplastic cells with hyperchromatic nuclei and indistinct cytoplasm. Frequent mitotic figures are evident and apoptotic nuclei may be encountered. A cytokeratin 20 stain is typically associated with a paranuclear dot-like pattern as seen in this case. CD56, neuron-specific enolase, as well as variable chromogranin, CD117, and synaptophysin staining are typically positive in most cases. A thyroid transcription factor (TTF) 1 stain is negative in most cases and helps exclude a diagnosis of a metastatic lung carcinoma, which can otherwise be associated with identical findings on routine histologic evaluation.
Which of the following is the typical immunophenotype for primary cutaneous CD8+ aggressive, epidermotropic, cytotoxic T-cell lymphoma?
CD8+, TIA-1+, TCRBF1+, CD5-
Sometimes referred to as “Berti’s lymphoma.”
In addition, unlike mycosis fungoides, this lymphoma is more likely to show expression of CD7 and loss of CD5.
The immunophenotype described in answer A is compatible with primary cutaneous g-DT-cell lymphoma. The immunophenotype described in answer C would be more typical of CD8+ mycosis fungoides than Berti’s lymphoma. Answer D is compatible with ALK+ systemic anaplastic large cell lymphoma. Answer E could be seen in adult T-cell lymphoma/leukemia, an HTLV-1 related neoplasm.
A 56-year-old woman has a red nodule on the ear that developed following trauma to the site. In view of the lack of clinical response to corticosteroids a punch biopsy was taken: the biopsy shows a dermal infiltrate with a vague nodular pattern. Small, medium and large lymphocytes are positive in a background of plasma cells and eosinophils. A Ki67 shows a low (<10%) proliferation index. Immunohistochemistry shows a mixture of T and B-cells. Frequent medium and large cells are positive for BCL-6, PD-1 and CXCL13.
On the basis of such findings, what is the most likely combination of pathologic diagnoses and clonality studies will be encountered?
Small to medium size CD4+ lymphoproliferative disorder; T-cell receptor clonal
Small to medium sized CD4+ lymphoproliferative disorder is an indolent provisional entity in the WHO that is characterized by a T-cell infiltrate with the expression of T-helper markers (BCL-6, CXL13, PD-1, ICOS) (E). Such lesions are invariably indolent. Additional staging procedures are not required for further evaluation. A rich background of B-cells is often noted, which can potentially mimic a CBCL.
Cutaneous marginal zone lymphoma does not show expression of BCL-6, CXCL13 or ICOS (A).
Unilesional mycosis fungoides is very rare and does not typically present in the face (B). A rich B-cell infiltrate is also not typical of mycosis fungoides.
Primary cutaneous follicle center lymphoma more typically manifests as a plaque (C). The lesions show a follicular or diffuse pattern. The neoplastic cells are B-cells with co-expression of BCL-6 and sometimes BCL-2. Immunoglobulin heavy is clonal in most cases.
Reactive lymphoid hyperplasia do not typically show an abundance of T-cells with TFH markers (D).

A 92-year-old woman develops three large nodules on the left leg. She reports that the nodules seemed to develop overnight. She has otherwise felt well. Immunohistochemical staining reveals strong expression of Bcl-2 and MUM1 in neoplastic cells (Figure).
Which of the following is the best diagnosis?
What are two possible treatments?

Primary cutaneous diffuse large B-cell lymphoma, leg type
The immunohistochemical staining with strong expression of Bcl-2 and MUM1 in neoplastic cells is characteristic of primary cutaneous diffuse large B-cell lymphoma, leg type. Cohesive sheets of centroblasts and immunoblasts are evident. The location on the lower legs is typical for primary cutaneous large B-cell lymphoma of the leg type. About one-quarter of all non-Hodgkin lymphoma cases present in an extranodal location without systemic involvement, with the skin being a common site. Fluorescence in situ hybridization reveals translocations of the MYC, Bcl-6, and IGH genes.
Treatment with rituximab is often helpful especially when combined with an anthracycline-based chemotherapeutic agent. Unfortunately, many patients have relapses.
A 42-year-old woman gradually developed a crusted lesion on the left medial thigh, an image of which is shown (Figure).
Which of the following is the best diagnosis?

Hemangioma with papillary endothelial hyperplasia (Masson tumor)
Intravascular papillary endothelial hyperplasia (Masson tumor) can occur within a dilated vascular space or in a preexisting hemangioma as in this case. Endothelial cells line vascular spaces and erythrocytes are noted within some of the vascular spaces.
A 37-year-old man with a long-standing history of mycosis fungoides developed multiple, ulcerative tumors.
Transformation to a large cell lymphoma (large cell transformation) in mycosis fungoides is defined as:

>25% of neoplastic T-cell are FOUR times the size of a normal lymphocyte
In CD30+ cases, the histopathologic differential diagnosis includes anaplastic large cell lymphoma (A); however, a clinical history of mycosis fungoides helps to exclude anaplastic large cell lymphoma in favor of CD30+, transformed mycosis fungoides. They may be CD30+ or CD30- (B). In diffuse large B-cell lymphoma, large cells are defined as twice the size of a normal lymphocyte (D) and form diffuse sheets of cells. While loss of CD7 by a large percentage of lymphocytes may help to establish a diagnosis of mycosis fungoides, this features is not used to determine large cell transformation (E).
A 40-year-old man with weight loss and kidney failure develops dusky nodules on the lower legs. A biopsy of one of the nodules was performed; the histopathologic features are shown in the image below.
Which of the following is the best diagnosis?

Polyarteritis nodosa
The biopsy specimen reveals a medium-sized artery with transmural inflammation. The segmental transmural inflammation of muscular arteries characterizes biopsies of polyarteritis nodosa. Polyarteritis does not involve veins. The infiltrate consists of polymorphonuclear leukocytes and mononuclear cells. Patients typically have associated fatigue, weight loss, weakness, fever, and arthralgias.
A 48-year-old man is being evaluated for multiple confluent plaques on the buttock area. The areas are pruritic and symmetrically distributed. A biopsy specimen is shown (Figure).
Which of the following is the best diagnosis?

Porokeratosis ptychotropica
Porokeratosis ptychotropica typically presents as multiple confluent plaques. Satellite areas of involvement may be noted and the lesions are often pruritic. Perianal involvement and symmetrical involvement of the buttocks is typical. Histopathology reveals multiple cornoid lamellae. Porokeratosis ptychotropica differs from porokeratosis of Mibelli in that the cornoid lamellae are multiple and somewhat irregularly distributed compared with the peripheral cornoid lamellae typical of porokeratosis of Mibelli.

A 72-year-old Caucasian man comes to clinic with a violaceous nodule on his scalp. Histologic findings are shown in the first image obtained. High power view demonstrates predominantly small lymphocytes. Immunohistochemistry for CD21 exhibited markedly enlarged, often disrupted and fused follicle dendritic cell networks (shown in the second image obtained). Lesional cells are diffusely positive for CD20, PAX-5, CD10, BCL-6, and BCL-2. MUM-1 is negative.
What is the best diagnosis?

Cutaneous involvement by nodal follicle center cell B-cell lymphoma
The histology shows dense nodular lymphocytic aggregates composed of small-sized lymphocytes with a bottom-heavy arrangement. Follicle center cell B-cell lymphoma (FCC-BCL) typically stains with BCL-6 and not BCL-2, however, the combination of BCL-6 and BCL-2 expression is highly suspicious for secondary cutaneous involvement by systemic (nodal) FCC-BCL. Primary FCC-BCL typically only stains with BCL-6, but not BCL-2.
OTOH, Marginal zone lymphoma (MZL-BCL) shows positivity with BCL-2, but not BCL-6.

An 87-year-old woman presents with multiple, rapidly growing violaceous lesions on her left lower leg (Figure 1). A biopsy demonstrates diffuse sheets of large lymphoid cells with rounded nuclear contours, open chromatin and visible nucleoli (Figure 2A, B).

CD20+, BCL2+, FOXP1+, MUM1+
Primary cutaneous diffuse large B-cell lymphoma, leg type is composed of sheets of large B-cells and is limited to the skin at diagnosis.
These large, round cells include centroblasts and immunoblasts, and differ from the irregular nuclei of centrocytes that are seen in primary cutaneous follicle center lymphoma. The neoplastic cells in primary cutaneous diffuse large B-cell lymphoma, leg type express BCL2, MUM1, IgM, and forkhead box protein 1 (FOX-P1) (B). BCL6 is common (68% of cases), but CD10 expression is not.

A skin biopsy from a 10-year-old boy shows the features in the first image obtained. Lesional cells are highlighted by CD1a.
Which additional immunohistochemical stains may be helpful in evaluating this patient?

CD207 (Langerin); G: S-100 and I:VE1 for BRAF V600E mutation

Langerhans cell histiocytosis (LCH) is characterized by the clonal expansion of CD1a+ CD207 (Langerin)+ S100+ Langerhans-type histiocytes (D, G). LCH cells appear to derive from bone marrow-derived immature myeloid dendritic cells and not from epidermal Langerhans cells. BRAF V600E mutation has been observed in a significant proportion of cases, predominantly younger patients without association with disease site or stage . The VE1 immunohistochemical stain identifies this specific mutation (I). CD5 is a T-cell marker (A); CD20 is a B-cell marker (B); CD138 is a plasma cell marker (C). Melan-A and Sox-10 are melanocyte markers (E, H). NSE is a marker of neural derivation (F).
Alopecia with “footprint in the snow” pattern is characteristic of what form of hair loss?

Pseudopelade of Brocq
A biopsy would show scarring alopecia including concentric perifollicular fibrosis, loss of sebaceous glands, and, eventually, loss of follicular units that are replaced by scar (end-stage scarring alopecia).
A 30-year-old woman comes to clinic with hair loss. A biopsy is performed. The findings are shown in the images obtained.
Given the histologic findings, what is the most likely clinical presentation in this case?

Patchy hair loss containing hairs with varying lengths
The images obtained depict a collapsed inner root sheath without hair shaft and a distorted narrow-caliber hair shaft (trichomalacia) with a pigment cast. These findings are pathognomonic for trichotillomania. Clinically, irregularly shaped patches of alopecia and hair shafts with varying lengths are characteristic (C).

A 48-year-old man presents with an 8 mm, asymptomatic pink papule on the scrotum of unknown duration. A shave biopsy is performed on the lesion and the histologic features are shown in the low and high power photomicrographs below.
Based on the images shown, what is the best diagnosis?

Verruciform xanthoma
The photomicrographs show digitate epidermal hyperplasia, overlying parakeratosis, and cornified and dyskeratotic cells within the surface crypts that appear to “float” into the scale. Numerous foamy macrophages are present within the papillary dermis, a feature which may be highlighted by a CD68 immunostain if necessary. The histologic findings are compatible with a verruciform xanthoma. Verruciform xanthoma is of unknown etiology, but may be related to minor trauma. It most commonly occurs on oral mucosae or anogenital skin. Although not seen in this example, the parakeratotic scale may have an orange hue on routine histology.

A five-year-old girl has multiple pedunculated and flat-topped papules on the dorsal hands with a predominant periungual location (Figure 1). Histopathology is shown (Figure 2).
Which of the following is the BEST diagnosis?
Will this be positive or negative for the following: CD68, factor XIIIa, S-100, and CD1a?

Multicentric reticulohistiocytosis
Multicentric reticulohistiocytosis is a very rare and aggressive condition characterized by skin lesions, mucosal lesions, and arthritis. It usually arises in middle-aged women. Histologic examination shows diffuse infiltration of the dermis by histiocytic cells and scattered multinucleated giant cells. The lesional cells demonstrate a dense pink cytoplasm, variously referred to as “oncocytic” or “ground glass.” The ground glass cytoplasm is periodic acid–Schiff positive. Immunostaining shows cell positivity for CD68 and factor 13a and negativity for S-100 and CD1a.

A 22-year-old woman presents with a solitary asymptomatic red plaque on the medial breast. A punch biopsy is performed with the histopathologic features shown in the low and high power photomicrographs below.
Which immunohistochemical stain is the most appropriate to confirm the diagnosis?

S100
At low power magnification, there is a diffuse dermal infiltrate creating a pattern of alternating dark and pale staining areas. At high power, the infiltrate is composed of large epithelioid histiocytes with abundant pale cytoplasms, lymphocytes, plasma cells, and neutrophils. Lymphocytes and neutrophils are present within the cytoplasms of the histiocytes, a phenomenon referred to as emperipolesis. Altogether, the histologic findings are compatible with a cutaneous manifestation of sinus histiocytosis (Rosai-Dorfman disease). The characteristic histocytes of Rosai-Dorfman disease show strong diffuse staining for S100, a result that can be particularly helpful when emperipolesis is subtle or the biopsy sample is small.
MART-1/Melan-A, Factor XIIIa, or CD1a would not help confirm the diagnosis as Rosai-Dorfman stains negative for these marker. CD68, while positive in Rosai-Dorfman, is a nonspecific marker of histiocytes.
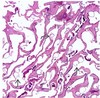
A 65-year-old man presents with tender, violaceous nodules on the lower extremities. A punch biopsy is performed on one lesion and the histologic features are shown in the low and high power photomicrographs.
Based on the images shown, what is the best diagnosis?

Pancreatic panniculitis
The photomicrographs show a large focus of robust fat necrosis, deposition of stippled basophilic material compatible with early calcification and numerous ghost cells characterized by central amorphous/granular debris rimmed by an eosinophilic membrane, findings that are compatible with pancreatic panniculitis. Although not seen in this example, there may also be an associated acute and chronic inflammatory infiltrate.
Calciphylaxis is characterized by variably apparent calcifications within small vessels in the subcutaneous tissue that are plugged with fibrin thrombi. A Von Kossa stain may help highlight the calcium. Usually, there is necrosis of the epidermis and/or dermis.
A 40-year-old woman comes to clinic with an asymptomatic umbilicated keratotic nodule on the face. The lesion is biopsied. The findings are shown in the image obtained.
What is the best diagnosis?

Warty dyskeratoma
Warty dyskeratoma is characterized by a central cup-shaped invagination, although cystic, nodular, and folliculocentric patterns have been reported. Within the deeper portion of the lesion villi are present. These villi project upward toward the surface and are lined by keratinocytes that show suprabasal acantholysis with cleft formation. Dyskeratosis is present with the formation of corp ronds and grains. Corp ronds are present within the upper stratum spinosum and stratum corneum and have a basophilic central pyknotic nucleus that is surrounded by a clear halo. Surrounding the halo is basophilic dyskeratotic material. Grains are smaller and resemble parakeratotic nuclei. Dyskeratotic material also surrounds the grains and can be either eosinophilic or basophilic. Grains are commonly seen in the stratum corneum.
Which of the following immunophenotypic findings are compatible with a diagnosis of primary cutaneous CD4+ small/medium T-cell lymphoproliferative disorder?
CD3+, CD4+, PD-1+, CD7-
Primary cutaneous small-medium pleomorphic T-cell lymphoma is an uncommon lymphoma that typically presents as a solitary, slowly enlarging and persistent nodule on the head, neck, or upper trunk. It is an uncommon lymphoma, but is a frequent histopathologic consideration in biopsies showing a dense, dermal lymphoid infiltrate without epidermotropism. It is characterized by a CD4-predominant T-cell infiltrate that expresses markers compatible with the immunophenotype of T-cells in the germinal/follicle center (also known as a follicular helper T-cell phenotype). These markers include BCL6, PD1, and CXCL13. In addition, this lymphoma often shows loss of one or more pan T-cell markers (ie, CD2, CD5, CD7) and a clonal T-cell population.
