Bone Metabolism Flashcards
What makes up the skeleton?
- Skeleton is 40% organic - predominantly type 1 collagen, but also non-collagenous proteins are present.
- 60% of it is inorganic (calcium hydroxyapatite)
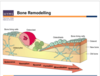
- Trabecular bone has a wide surface area, structure which is mechanically strong.
- Trabecular bone is actually a target area for bone remodelling.
- Those bite marks you see are resorption pits.

What would you find it you were to look close up at the resorption pits?
- You’d see osteoclasts and osteoblasts.
- You can see the osteoclast sitting in the resorption pit, removing away the bone.
- Osteoblasts are mononuclear single nucleotide cells (cuboidal cells) which produce type-1 collagen and new bone matrix (unmineralised)
- Some osteoblasts bury themselves alive (in the red bit) in the bone matrix, and become osteocytes in the bone matrix.

Give an overview of bone remodelling.
- Resorption - osteoclasts arrive at the bone surface and start to resorb the stuff.
- Then reversal phase, switch from absorption to formation (osteoblasts lay down initially un-mineralised type-1 collagen) and later on that becomes mineralised to bone.
- Then finally, calcium ion released into system.
What signalling mechanisms are involved in controlling cells that can affect calcium levels in circulation?
What is bone matabolism?
- Bone metaboism drives bone remodelling.
- Maintains levels of ionised calcium in blood within a defined range.
- Signalling mechanisms include:
- Parathryoid Hormone (PTH)
- 1,25 (OH)2 vitamin D3
- Calcitonin
- Growth Hormone
- Growth Factors (FGFs, TGFs)
- Oestrogen
- Cytokines (e.g. Interleukin-1, interferon-y)
What should serum concentration of calcium be at?
- Reccomended daily intake - 1000mg
- 99% of calcium in skeleton
- 1% in extracellular fluid and soft tissues
Serum Concentration of calcium = 2.25-2.6mmol/L
What are the three forms of calcium found in serum?
- Ionised calcium (Ca2+) (about 50% of all calcium).
- Protein-bound calcium (primarily to albumin - 40%)
- Complexed calcium (mostly to citrate and phosphate, 10%)
It is the ionised calcium that is physiologically important.
Ca2+ ion levels are maintained by PTH, vitamin D, calcitonin (+ others)
What are the three definable fractions of inorganic phosphate int he serum:
- Ionised phosphate (55%)
- Protein-bound phosphate (10%)
- Complexed phosphate (mostly to sodium, calcium and magnesium).
What regulates phosphate levels?
- Parathyroid Hormone (PTH)
What are the usual levels of phosphate?
- Major ionic species of phosphate in serum at pH 7.4 is the divalent anion (HP042-)
In contrast to rigid regulation of calcium levels, phosphate concentrations in serum vary quite widely, influenced by age, diet, pH, hormones.
Usually around 0.9-1.3 mmol/L.
How much phosphorus is found in the adult human body?
- Approximately 600g
- 85% in the skeleton
- 15% in extracellular fluids, largely in the form of inorganic phosphate ions.
How is vitamin D synthesised?
Vitamin D is synthesised from cholecalciferol.
Synthesised in skin from 7-dehydrocholesterol.
25-hydoxylation in the liver produces 25(OH)D3 - the main circulating metabolite with little biological activity.
1-hydroxylation in the kidney produces 1,25 (OH)2 vitamin D3

What is the principal hormonal form of Vitamin D?
1,25 (OH)2 Vitamin D3
This is the principal hormonal form of Vitamin D and is responsible for most of its biological actions.
1,25(OH)2 vitamin D3 production is tightly regulated and stimulated by PTH and inhibited by elevated serum Calcium and Phosphate.

What actions does 1,25(OH)2 Vitamin D3 engage in?
- It increases calcium and phosphate absorption from the intestine.
- It mobilises calcium and phosphate from bone.
- It induces marrow monocytes to differentiate into osteoclasts to stimulate born resorption.

What are the vitamin D3 metabolites?
- 24-hydroxylation of 25(OH)D3 and 1,25(OH)2D3 produces 24,25(OH)2D3 and 1,24,25 (OH)3D3
- 24-hydroxylation generally first stage in catabolism of active vitamin D metabolites.
- 24-hydroxylase is induced by 1,25(OH)2D3 which produces a feedback mechanism to prevent vitamin D toxicity.
- 24,25(OH)2D3 and 1,24,25 (OH)3D3 biological activities unclear.

What is Parathyroid Hormone? (PTH)
- It is an 84 amino acid polypeptide.
- Molecular weight 9,500
- Half-life: 20 minutes.
‘It is secreted by the parathyroid gland in response to low plasma Ca2+ levels.’

What are the actions of PTH?
- Stimulate osteoclastic bone resorption, therefore mobilises calcium from bone.
- Intermittent low levels of PTH appear to stimulate osteoblastic bone formation.
- PTH mediates its effects predominantly through osteoblasts, which communicate directly with osteoclasts to transmit PTH-dependent effects on resorption.
- Decreases renal calcium excretion
- Increases renal production of 1,25(OH)2 Vitamin D3.
- Increases blood calcium levels.

Explain the role of Calcitonin
- Calcitonin is a 32 amino acid polypeptide.
- It is released from the parafollicular (C) cells of the thyroid in response to high plasma calcium levels (>2.25mmol/L).
- Reduces bone resorption by activating calcitonin receptors expressed by osteobclasts.
Explain the process of calcium metabolism.
- Decreased in Ca2_ induces PTH secretion, which mobilises calcium (bones), decreases renal calcium excretion and increases renal synthesis of 1,25(OH)2D3 that also enhances calcium mobilisation and absorption (bones, intesine).
- Increased Ca2+ increases calcitonin secretion (inhibits bone resorption) and decreases 1,25(OH)2D3 synthesis.

What are the clinical features of Osteomalacia and Rickets?
- Diffuse bone pain
- Localised bone pain around hips
- Muscle weakness.
- Elevated alkaline phosphatase levels.
- Decreased mineralisation.
- Weight bearing long bones display a bowing demormity

What treatment options are there for Osteoporosis?
- Calcium supplementation
- Hormone Replacement Therapy (HRT)
- Biophosphates (potent inhibitors of boen resorption, Alendronate, Residronate, Etidronate).
- Calcitonin
- Selective Estrogen-Receptor Modulator (SERMs) - produces oestrogen agonist effects slectively in bone Raloxifene.
