14.1 Eye disease Flashcards
What is required for us to be able to see?
- Eye
- Clear cornea
- Clear lens
- Functioning retina and optic nerve
- Brain
- LGN (lateral geniculate nucleus)
- Superior colliculus
- Edinger-Westphal nucleus
- III nucleus
- IV nucleus
- VI nucleus
-
Frontal lobe (voluntary eye movements)
- Causes body movements
-
Vestibular nuclei
- Gaze stabilisation
-
Occipital lobe
- Pursuit eye movements & accomodation
- Dorsal stream (where it is?)
- Ventral stream (what it is?)
- CN III, IV, VI

What do different areas of the eye do?
- Cornea = refraction
- Lens = focussing
- Iris = controlling amount of light entering the eye
- Retina = phototransduction
- Optic nerve = carrying electrical signals to the brain

What is the function of the cornea & the layers?
- Main function is refraction
- 5 layers
- NO blood vessels but can grow but affect vision
- O2 (oxygen) from the atmosphere

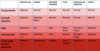
What is normal refraction called and give examples of refractive errors and how to correct them?

What is astigmatism & explain it
- Cornea is not spherical
- Different radii of curvature in different axes
- In this case the vertical radius is shorter than the horizontal radius therefore the curvature of the cornea is steeper in the vertical axis than the horizontal axis.
- To correct this a cylindrical lens is needed with different powers in the different axes.
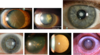
List some corneal diseases
- Corneal ulcer
- Corneal dystrophy
- Keratoconus
- Corneal oedema
What is this & explain it

CORNEAL ULCER
- Usually due to poor hygiene in contact lens wearers
- Can be treated with antibiotics
What is this?

Corneal dystrophy (rare)
What is this?

Keratoconus
- Treatment with corneal graft (given to allow good vision)
What is this?

Corneal oedema
- Due to failure of endothelial pumps
- Treatment with corneal graft
What is this?

Corneal graft
- Given to allow good vision
Explain what happens in the lens
- Some refraction
- Accommodation/fine focus:
- Circumferential ciliary muscle contracts allowing lens capsule to relax, lens becomes more spherical
- As we age this gets worse

What is cataract & what are the risk factors & treatment?
- Cataract: clouding of the lens
- Risk factors:
- Age
- Diabetes
- Corticosteroids
- Congenital
- Trauma
- Treatment
- Can be treated by surgery
What is this condition?
Cataracts
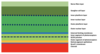
What are all the layers in the retina?
Inner at top
Outer at bottom (photoreceptors where transduction occurs)
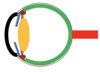
What is the blood supply to the retina?
Blood from:
-
Central retinal artery
- Supplies innermost layers
-
Choroid artery
- Supplies outermost layers
What is the imaging of this picture?

Optical coherence tomography
What is the foveal dip?
- Where light entering the eye causes the sharpest image
- Increase in visual acuity
- Increase in determination of colour
-
Fovea appears slightly darker as it is thinnest here
- Choroid is most visible
- Hence, light can get straight to photoreceptors

What is the concentration of rods & cones in the retina?
-
RODS
- 6.5 million
- Increase numbers at the fovea
-
CONES
- 120 million
- None at fovea
- Widely spread throughout the retina
-
OPTIC DISC
- NO photoreceptors at the optic disc
Explain photoreceptors & the structure of them
- Photoreceptors is where phototransduction occurs
- Rods = scotopic vision (vision under LOW light levels)
- Cones = photopic vision (vision under WELL-lit conditions)
-
DISKS hold opsin molecules
- Rhodopsin in rods
- Iodopsin in cones
- Light stimulates the isomerisation of retinal which activates opsin leading to hyperpolarisation of the photoreceptor
-
3 different opsins present in all cones but one predominates in each of three different cones:
- “Blue” cones containing mostly blue-sensitive opsin are excited chiefly by a wavelength of around 420 nm,
- “Green” cones by a wavelength around 530 nm,
- “Red” cones by a wavelength near 560 nm

Explain phototransduction in detail

Role of ON-OFF switches in phototransduction
- Are to do with the modification of signal by transduction
List some retinal diseases
- Colour blindness
- Retinal vascular occlusion
- Diabetes
- Macular degeneration
- Retinal detachment
Explain colour blindness & how it can be tested
- There are many forms of colour blindness
- Depends on which cones are affected (total loss/do not function properly)
- Red-Green colour blindness is the most common type
- Naming of colour blindness:
- Prot- = Red (L) cones
- Deuter- = Green (M) cones
- Trit- = Blue (S) cones
- -anomaly = malfunctioning
- -anopia = absent
- Tested
- Using the Ishihara test plates
Explain central retinal artery occlusion (CRAO)
- Common in diabetes & hypertension
- Causes the inner retinal cells to die
- If retina loses blood supply then the retina thins as cells die
- Vision is very poor
- Sudden or total visual loss

What is diabetic retinopathy & treatment
- Small blood vessels leak or get blocked (forming micro-aneurysms)
- Leads to oedema, exudation and haemorrhage in inner retinal layers
- Worse diabetes = INCREASE likely to have this
- Treatment
- With anti-VEGF injections/steroids

What is wet age-related macular degeneration?
- Inflammation & hypoxia due to aging eye (forms INCREASE VEGF)
- New blood vessels grow from the choroid through the retinal pigment epithelium
- These leak and bleed causing oedema and haemorrhage in the outer retinal layers
- This causes distorted vision as photoreceptors are displaced
*

Why do you get a distorted image with wet ARMD (age related macular degeneration)?
- Pixels: Each cone is responsible for seeing one part of the face and that is mapped exactly in the occipital cortex
- If oedema separates the cones their pixels will be different
- The brain assembles the image as though cones are in correct place therefore image appears distorted

What is retinal detachment & symptoms & treatment for it?
- Posterior vitreous detachment (PVD)
- Vitreous remains attached to part of the retina, the traction causing a tear
- Fluid breaks through the break in the retina between the photoreceptor layer and the retinal pigment epithelium
- Fluid continues to leak thanks to gravity creating a retinal detachment
Symptoms
- Flashing lights
- Potential shadow in vision
Treament
- Retina reattached ASAP
- As photoreceptors NOT recieving adequate blood supply

What is the blood supply to the optic nerve?

What is glaucoma & the treatment for it?
- Progressive optic neuropathy causing the loss of the nerve fibre layer causing CUPPED OPTIC DISC appearance and corresponding VISUAL FIELD DEFECTS
- Commonly associated with raised INTRA-OCULAR PRESSURE
- Causes field loss depending on which part of the optic nerve is damaged the most
-
TREATMENT
- Various topical drops
- Surgery (more serious cases)

What is anterior ischaemic optic neuropathy & treatment?
- When branches of posterior ciliary arteries are affected
- Most commonly due to microvascular occlusion related to diabetes, hypertension, atherosclerotic disease , but can be due to inflammatory causes including Giant Cell Arteritis (serious rheumatological disease where: losing appetite & feeling very unwell & pain in jaw & hard to comb hair as scalp tender)
-
NOT caught early enough = VISUAL loss can occur –> IRREVERSIBLE
- Once 1 eye blind INCREASE likely without treatment other eye can become blind
-
TREATMENT
- HIGH dose of steroids

What is thyroid eye disease & treatment?
- Inflammation of the extra-occular muscles & proptosis (forward movement of eye)
-
TREATMENT
- Steroids
- Radiotherapy
- Surgery

What is orbital cellulitis & treatment?
- Inflammation of eye tissues behind the orbital septum. It is most commonly caused by an acute spread of infection into the eye socket from either the adjacent sinuses or through the blood
- Usually in children
- Causes protosis & optic nerve compression
-
TREATMENT
- Imaging
- Surgery

What conditions can stop us from seeing & the areas that they affect?
- Corneal opacity
- Cataract
- Optic neuritis
- Glaucoma
- AION
- Optic nerve compression
- CRAO
- Retinal detachment
- Wet ARMD
- Diabetic maculopathy
What comprises the visual pathway and explain where in the brain (diagram)?

Where can visual field defects occur and explain what they cause?
Pituitary lesions –> damage to optic chiasm = bitemporal hemianopia

What happens to the electrical signals from the optic nerve (draw this as a diagram)?
-
Occipital lobe = allows us to focus on moving things
- Pursuit eye movements & accomodation
- Sends messages to LGN & superior colliculus & Edinger-Westphal nucleus
- These send messages to III nucleus, IV nucleus, VI nucleus which control eye movements
-
Vestibular nuclei
- Gaze stabilisation so, allows our surroundings to stay still whilst we move
- When drinking/ear infection this can be affected
-
Ventral stream
- Pathway from occipital lobe to temporal lobe
- Responsible for interpreting WHAT we see
- Recognition of objects, facial recognition, colour memory
-
Dorsal stream
-
WHERE is it?
- Spatial awareness, looking for things
- From the occipital lobe to the frontal lobe
-
WHERE is it?
-
Frontal lobe
- Voluntary eye movements
- Connects to motor cortex & enables us to respond appropriately
- WHAT we gonna do about it? e.g. run away from fire

What are the eye muscles & what nerve are they innervated by?
III nerve = SR, IR, MR, IO
IV nerve = SO
VI nerve = LR

What is the accommodation reflex & explain its pathway
- Causes eyes to converge thanks to III nerve (short ciliary nerve from ciliary ganglion)
- Causes pupil constriction & accommodation of lens
Pathway:
- Visual cortex
- to EW ganglion
- to PS fibres
- to Ciliary ganglion
- to Short ciliary nerve
Pupil constriction:
- Circumferential muscle fibres in the iris contract. Pupil becomes smaller
Accommodation of lens
- Circumferential ciliary muscles contract, zonules relax and elastic capsule of lens relaxes. Lens becomes more spherical

Explain pupil responses and the different types of innervation & drugs that can allow these responses to happen
- Pupil responds to light –> NO involvement of visual cortex
- Fibres from optic tract peal off at Pre-tectal ganglion then decussate into Edinger-Westphal ganglion
- To the ciliary ganglion via the short ciliary nerve
- Constriction of pupil (BILATERAL)
- Abscence of light = puppils dilate again
- Active DILATING due to sympathetic innervation (NA - noradrenaline)
- Useful for examining fundus
- Phenylephrine –alpha 1 agonist (dilates)
Tropicamide, Cyclopentolate, Atropine - cholinergic antagonists
(dilate and reduce accommodation)
- Active CONSTRICTION due to parasympathetic innervation (ACh - acetylcholine)
- Pilocarpine-cholinergic agonist

What is blindsight & explain this
- As goes via this pathway we are NOT consciously aware of it
- Bilateral occipital damage demonstrates blindsight

Explain the mechanism of pain (types and types of pain receptors)
TYPES OF PAIN (in eye)
-
Nociceptive
- Damage to non-neural tissue
-
Neuropathic
- Damage to nerve
-
Inflammatory
- Activation of nociceptors by inflammatory mediators
-
Sudden raised Intra-ocular pressure
- Activation of nociceptors by ATP
TYPES OF PAIN RECEPTORS (in eye)
- Found on surface of eye, conjunctiva, cornea, anterior chamber & iris
- LENS & RETINA = NO nerve fibre endings for pain

What areas of the eye would have to be examined in order to find the cause of pain? (& what device would you use?)
- Eyelids
- Conjunctiva
- Cornea
- Anterior Chamber
- Iris
Can examine these using a slit lamp

Draw the anatomy of the eyelid & annotate it

What is blepharitis & the treatment for it?
- Inflammation of eyelids
- Is squamous type
- Very common
TREATMENT
- Warm compresses
- Lid hygiene

What is meibomianitis & the treatment for it?
- Inflammation of meibomian glands (OR blocked = excess secretion formes and DISTURBS tear film
- Sebaceous type
- Very common
TREATMENT
- Warm compresses
- Lid hygiene

What are the different types of lumps & bumps on the eye and briefly explain them & treatment for one
-
CYST OF MOLL (left pic)
- Blocked gland of Moll (modified sweat gland)
-
STYE (middle pic)
- Blocked sebaceous gland related to hair follicle
-
CHALAZION (right pic)
- Blocked meibomian gland
- In tarsal plate thus, secretions formed and causes lump
-
Treatment
- Massaging eyelid (opens up Meibomian glands)
- Warm compresses
- Surgery (severe)

What is entropian, ectropion & trichiasis?
-
ENTROPION (left pic)
- Eyelid turned in (as loose), lashes rubbing on cornea (pain, treatment needed)
- Usually when people get OLDER (as less orbital fat) and less tension in muscles acting on eyelid
-
ECTROPION (middle pic)
- Eyelid turned out (less painful)
- Usually when people get OLDER (as less orbital fat) and less tension in muscles acting on eyelid
-
TRICHIASIS (right pic)
- Lashes turned in rubbing on cornea (eyelid in incorrect position)

What are some lid diseases & what happens to the lashes, lid position & what glands are involved?

What are some conjunctiva diseases?
-
BACTERIAL CONJUNCTIVITIS (top left)
- Sticky discharge
- Lasts 3-4 days
-
VIRAL CONJUNCTIVITIS (bottom left)
- Watery discharge
- Lasts many weeks
-
ALLERGIC CONJUNCTIVITIS (right)
- Chemosis
- Lid changes

Where can foreign bodies enter in the eye?
- SUB-TARSAL FOREIGN BODY (left)
-
CORNEAL FOREIGN BODY (right)
- Usually due to high speed injuries e.g. drilling

What are the layers of the cornea and briefly describe them
Main function of the cornea is refraction
-
Epithelium
- Several layers of cells
- Barrier to water and bacteria entering the cornea
- Maintains a smooth optical surface for refraction
- Bowman’s layer
- Stroma (keratocytes)
- Descemet’s membrane
-
Endothelium
- Single layer of hexagonal cells
- Allows transport of nutrients including glucose into the cornea
- Pumps water out to maintain clarity of stroma

What are some common corneal problems?
-
DRY EYES (top left)
- Aqueous part of tear production NO longer working adequately as epithelial cells start dying off
-
CORNEAL ABRASION (bottom left)
- Painful
- e.g. poked in the eye
- DENDRITIC ULCER (HSK) (top right)
- BACTERIAL ULCER (bottom right)
Fluorescein is used to show epithelial defects
Explain how the anterior chamber of the eye works & label (draw)
-
Ciliary body
- Produces aqueous component which circulates
- When blocked = INCREASEin pain
- Produces aqueous component which circulates
-
Trabecular meshwork
- Aqueous component leaves via here into venous system

What are the symptoms of acute angle closure glaucoma? (AACG)
- Severe pain (ATP mediated)
- Vomiting
-
Reduced vision
- As aqueous has nowhere to go thus, through cornea and becomes water logged
- Rainbow haloes (corneal oedema-altered refraction of light)

What is the mechanism of AACG?
-
HYPERMETROPIA (usually occurs in these people)
- Long sight-smaller eyes
- Shallower AC
- Enlarged lens (when older)
- Pupil dilates in low light
- Iris sticks to enlarged lens
- Aqueous cannot flow in to AC pushes iris forward
- Iris closes off already narrowed angle
- IOP rises

What does the uveal tract consist of?
- Iris
- Ciliary body
- Choroid

What is acute anterior uveitis? & treatment?
- Is the inflammation of the iris which can cause the eye to become red
- Can be idiopathic or related to auto-immune or other inflammatory conditions
- Treatment includes steroids & dilating drops where iris has got stuck to the lens
- Iris stuck to lens (posterior synechiae)

What conditions could cause a red eye?
When DECREASED vision &/OR photophobia = INCREASE serious condition